The nurse is caring for a 4-month-old infant in the emergency department. The nurse reviews the infant's medical record and assessment findings. Which of the following conditions should the nurse suspect, and what actions should the nurse take to address that condition, and what parameters should the nurse monitor to assess the infant's progress?
The nurse should suspect that the infant has
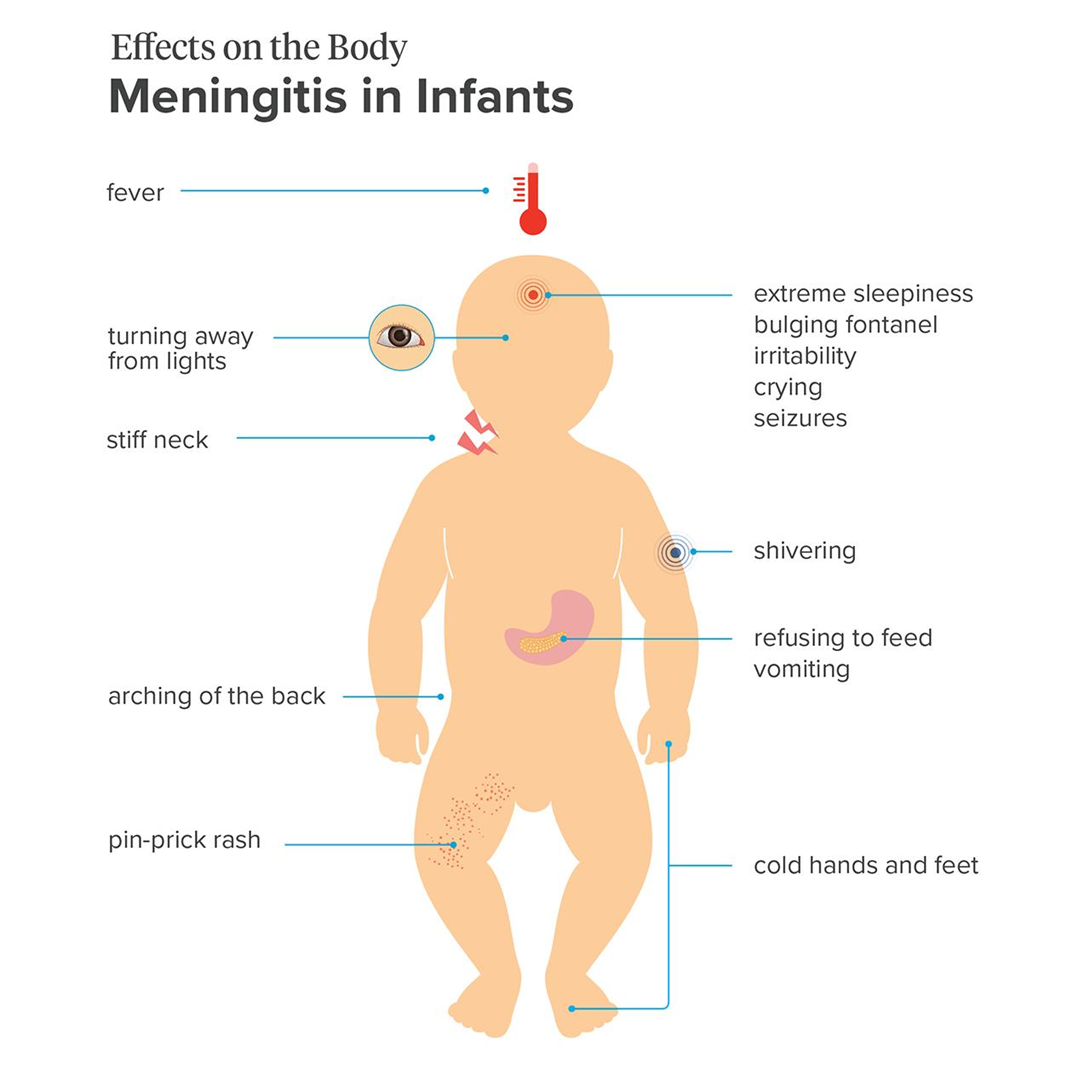
meningitis.
hydrocephalus.
intracranial hemorrhage.
sepsis.
The Correct Answer is A
Choice A reason: Meningitis is a possible condition, as it is an inflammation of the membranes that cover the brain and spinal cord. It can be caused by various microorganisms, such as bacteria, viruses, or fungi. The infant has many signs and symptoms of meningitis, such as fever, irritability, lethargy, bulging fontanel, and clear cerebrospinal fluid from the lumbar puncture.
Choice B reason: Hydrocephalus is not a likely condition, as it is an accumulation of cerebrospinal fluid in the brain, which causes increased intracranial pressure and enlargement of the head. The infant has a bulging fontanel, which can indicate increased intracranial pressure, but not necessarily hydrocephalus. The infant does not have other signs of hydrocephalus, such as a rapidly increasing head circumference, prominent scalp veins, or sunset eyes.
Choice C reason: Intracranial hemorrhage is not a probable condition, as it is a bleeding within the skull, which can result from trauma, vascular malformation, or coagulation disorder. The infant has retinal hemorrhages, which can indicate intracranial hemorrhage, but not necessarily. The infant does not have other signs of intracranial hemorrhage, such as seizures, vomiting, or altered mental status.
Choice D reason: Sepsis is not a definite condition, as it is a systemic inflammatory response to an infection, which can cause organ dysfunction and shock. The infant has a fever, which can indicate sepsis, but not necessarily. The infant does not have other signs of sepsis, such as tachycardia, tachypnea, hypotension, or poor perfusion.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: A 2-year-old toddler is not a recommended recipient of the MCV4 vaccine, as it is not routinely given to children younger than 11 years old, unless they have certain medical conditions that increase their risk of meningococcal disease, such as asplenia, complement deficiency, or HIV infection. A 2-year-old toddler may receive the meningococcal polysaccharide (MPSV4) vaccine instead, if indicated.
Choice B reason: A 4-month-old infant is not a recommended recipient of the MCV4 vaccine, as it is not routinely given to children younger than 11 years old, unless they have certain medical conditions that increase their risk of meningococcal disease, such as asplenia, complement deficiency, or HIV infection. A 4-month-old infant may receive the meningococcal serogroup B (MenB) vaccine instead, if indicated.
Choice C reason: An 11-year-old school-age child is a recommended recipient of the MCV4 vaccine, as it is routinely given to children aged 11 to 12 years old, with a booster dose at age 16. The MCV4 vaccine protects against four types of meningococcal bacteria (A, C, W, and Y) that can cause serious infections of the lining of the brain and spinal cord (meningitis) or the bloodstream (septicemia).
Choice D reason: A 4-year-old child is not a recommended recipient of the MCV4 vaccine, as it is not routinely given to children younger than 11 years old, unless they have certain medical conditions that increase their risk of meningococcal disease, such as asplenia, complement deficiency, or HIV infection. A 4-year-old child may receive the meningococcal polysaccharide (MPSV4) vaccine instead, if indicated.
Correct Answer is ["C","D"]
Explanation
Choice A reason: Loss of appetite is not an urgent finding, as it may be caused by various factors, such as nausea, pain, or stress. The nurse should monitor the child's fluid and calorie intake and encourage oral hydration and nutrition. However, loss of appetite does not require immediate reporting to the health care provider.
Choice B reason: Platelet count is not an urgent finding, as it is not given in the text. The nurse should check the child's laboratory results and compare them with the normal ranges for preschoolers. A normal platelet count for children is 150,000 to 450,000 per microliter of blood¹. A low platelet count (thrombocytopenia) may indicate bleeding disorders, infections, or bone marrow problems. A high platelet count (thrombocytosis) may indicate inflammation, infection, or cancer. The nurse should report any abnormal platelet count to the health care provider, but it is not an immediate concern.
Choice C reason: Developmental regression is an urgent finding, as it may indicate a serious neurological problem, such as a brain tumor, infection, or injury. Developmental regression is the loss of previously acquired skills or milestones, such as language, motor, or social skills. The nurse should assess the child's developmental level and report any signs of regression to the health care provider as soon as possible.
Choice D reason: Absolute neutrophil count is an urgent finding, as it may indicate a severe infection or a compromised immune system. Neutrophils are a type of white blood cell that fight bacterial infections. The absolute neutrophil count is the number of neutrophils in a microliter of blood. A normal absolute neutrophil count for children is 1,500 to 8,000 per microliter of blood². A low absolute neutrophil count (neutropenia) may increase the risk of infection and sepsis. A high absolute neutrophil count (neutrophilia) may indicate an acute infection or inflammation. The nurse should report any abnormal absolute neutrophil count to the health care provider immediately.
Choice E reason: Hemoglobin is not an urgent finding, as it is not given in the text. The nurse should check the child's laboratory results and compare them with the normal ranges for preschoolers. Hemoglobin is a protein in red blood cells that carries oxygen. A normal hemoglobin level for children is 11.5 to 15.5 grams per deciliter of blood³. A low hemoglobin level (anemia) may indicate blood loss, iron deficiency, or bone marrow problems. A high hemoglobin level (polycythemia) may indicate dehydration, lung disease, or heart disease. The nurse should report any abnormal hemoglobin level to the health care provider, but it is not an immediate concern.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today