A nurse is creating a plan of care for a child who has sickle cell anemia. Which of the following interventions should the nurse include in the plan?
Discourage a high level of fluid intake.
Administer meperidine every 4 hr for pain.
Apply cold compresses to painful, swollen joints.
Observe for indications of hypokalemia.
The Correct Answer is D
Choice A reason: Discouraging a high level of fluid intake is incorrect, as hydration is essential for preventing sickle cell crises and reducing blood viscosity. The nurse should encourage the child to drink at least 1.5 times the normal fluid requirement.
Choice B reason: Administering meperidine every 4 hr for pain is incorrect, as meperidine is not recommended for sickle cell pain due to the risk of neurotoxicity and seizures. The nurse should use other opioids such as morphine or hydromorphone for pain management.
Choice C reason: Applying cold compresses to painful, swollen joints is incorrect, as cold can cause vasoconstriction and worsen the sickling of red blood cells. The nurse should use warm compresses or heating pads to promote vasodilation and blood flow.
Choice D reason: Observing for indications of hypokalemia is correct, as sickle cell anemia can cause hemolysis and potassium loss. The nurse should monitor the child's serum potassium level and watch for signs of hypokalemia such as muscle weakness, cramps, arrhythmias, and constipation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
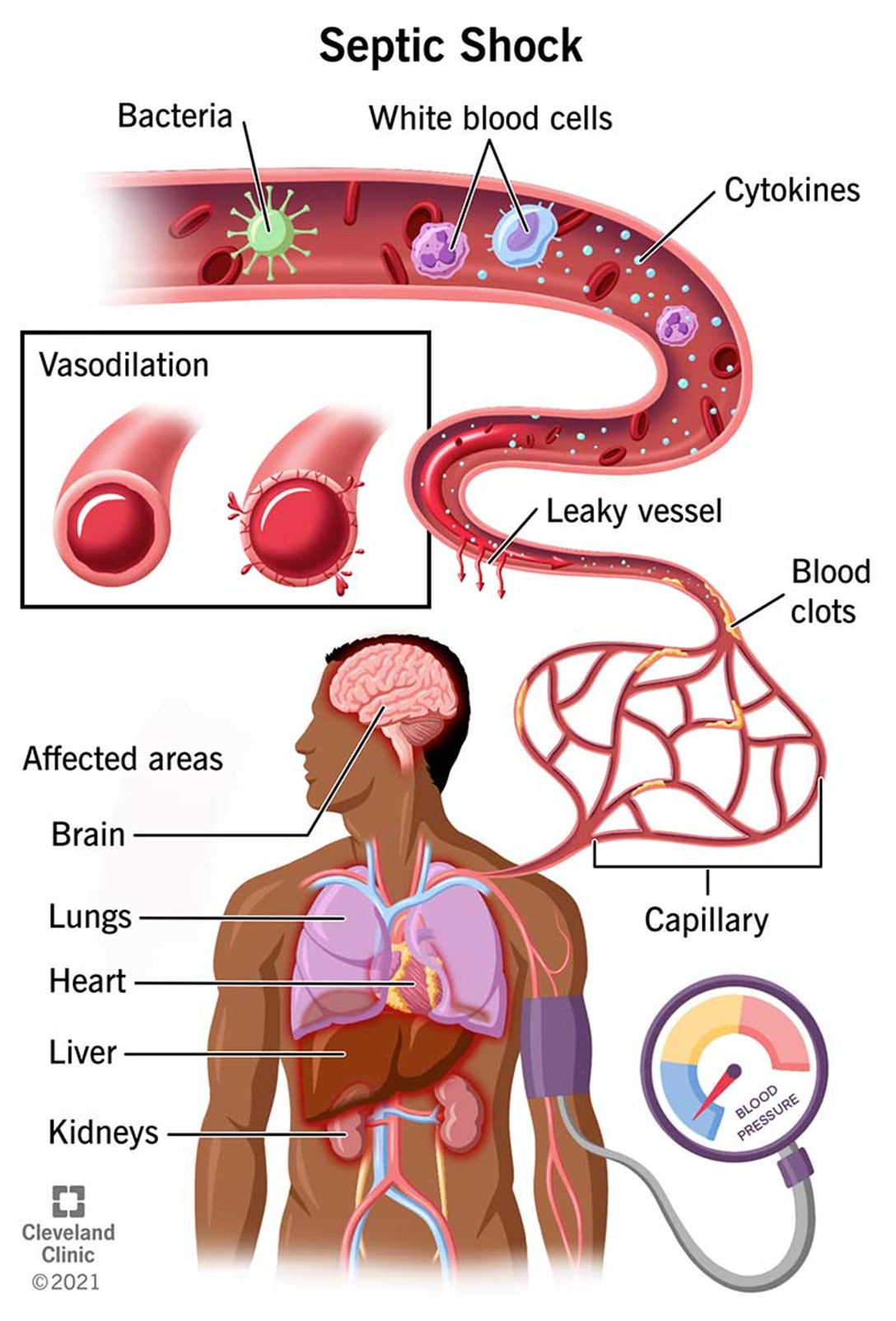
Choice A reason: Broad-spectrum antibiotics are indicated for septic shock caused by bacterial infection, as they can target a wide range of pathogens and prevent further sepsis. Fluid boluses are also essential to restore the intravascular volume and improve tissue perfusion and oxygenation.
Choice B reason: Antipyretics and oxygen therapy are not sufficient to treat septic shock, as they do not address the underlying infection or the hypovolemia. Antipyretics may lower the temperature, but they do not eliminate the bacteria. Oxygen therapy may improve the pulse oximeter reading, but it does not correct the hypoperfusion.
Choice C reason: Vasopressors and blood transfusions are not the first-line treatments for septic shock, as they may have adverse effects on the cardiovascular system and the coagulation cascade. Vasopressors may increase the blood pressure, but they may also cause vasoconstriction and reduce the blood flow to vital organs. Blood transfusions may increase the hemoglobin level, but they may also increase the risk of fluid overload, hemolysis, and transfusion reactions.
Choice D reason: Corticosteroids and antihistamines are not indicated for septic shock, as they do not have any proven benefits and may have harmful effects on the immune system and the inflammatory response. Corticosteroids may suppress the adrenal function and increase the risk of infection. Antihistamines may cause sedation and dryness of the mucous membranes.
Correct Answer is C
Explanation
Choice A reason: Failure to thrive is not a likely condition, as it is a term used to describe inadequate growth or weight gain in children. The infant has a low weight percentile, but not below the 5th percentile, which is the usual cutoff for failure to thrive. The infant's length and head circumference are within the normal range, which also does not indicate failure to thrive.
Choice B reason: Microcephaly is not a probable condition, as it is a condition where the head size is much smaller than normal for the age and sex of the child. The infant has a high head circumference percentile, which is the opposite of microcephaly. Microcephaly can be caused by genetic disorders, infections, or brain damage.
Choice C reason: Hydrocephalus is a possible condition, as it is a condition where excess cerebrospinal fluid accumulates in the brain, causing increased pressure and enlargement of the head. The infant has a high head circumference percentile, which can indicate hydrocephalus. The infant also has a low weight percentile, which can be a result of poor feeding or vomiting due to increased intracranial pressure. T
Choice D reason: Macrocephaly is not a definite condition, as it is a term used to describe a head size that is much larger than normal for the age and sex of the child. The infant has a high head circumference percentile, but not above the 97th percentile, which is the usual cutoff for macrocephaly. Macrocephaly can be caused by genetic factors, benign familial macrocephaly, or other conditions, such as hydrocephalus.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today