A patient is admitted for pain in the arm and jaw. The patient is later diagnosed with angina.
What type of pain does the arm and jaw pain most likely represent?
Intractable
Phantom
Referred
Cramping
The Correct Answer is C
Choice A rationale:
Intractable pain is pain that is persistent and does not respond to usual pain management methods. While angina can be intractable in some cases, it does not typically manifest as pain in the arm and jaw. Moreover, the patient in this scenario has not yet undergone pain management efforts, so it's premature to classify the pain as intractable.
Choice B rationale:
Phantom pain is pain that is felt in a part of the body that has been amputated or is no longer there. The patient in this scenario has not experienced any amputations, so phantom pain is not a valid explanation for the arm and jaw pain.
Choice C rationale:
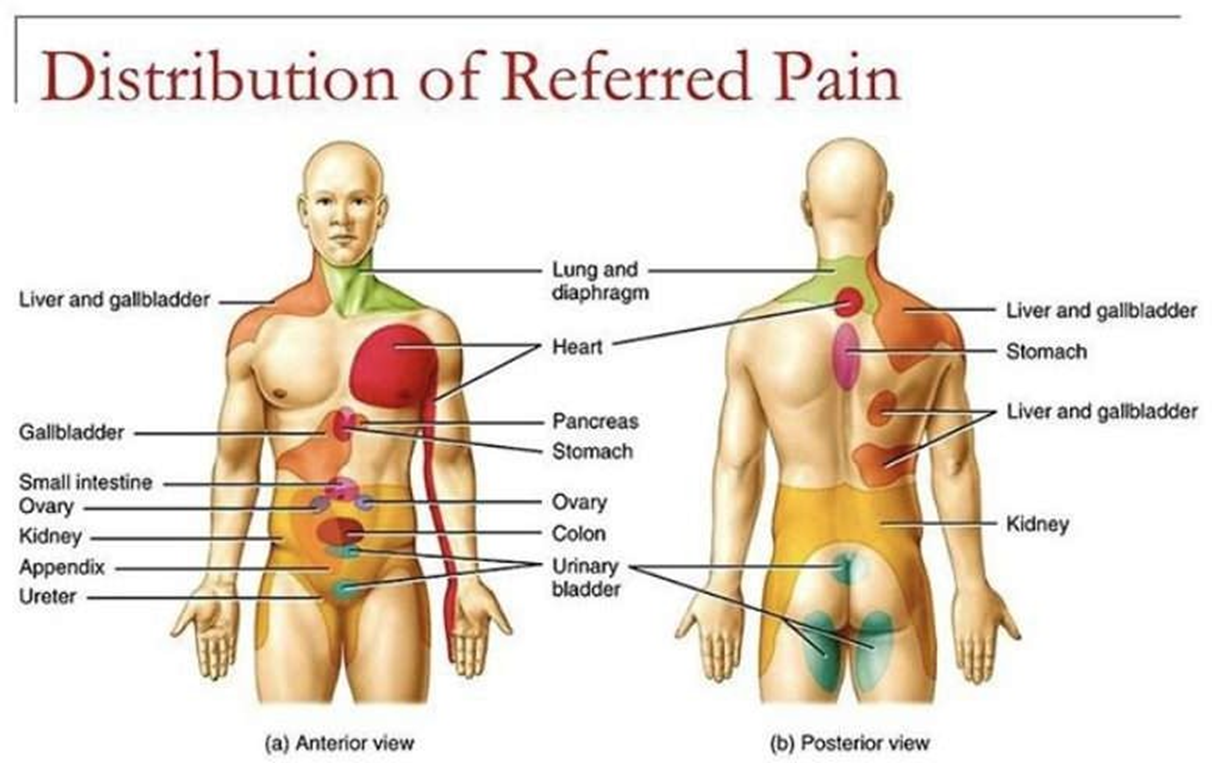
Referred pain is pain that is felt in a part of the body that is different from the source of the pain. This is the most likely explanation for the arm and jaw pain in this patient. The heart and the arm and jaw share nerve pathways, so pain signals from the heart can be misinterpreted by the brain as coming from these other areas. This is a common phenomenon in patients with angina.
Choice D rationale:
Cramping pain is a type of pain that is often described as a muscle tightening or squeezing sensation. It is not typically associated with angina. While angina can sometimes cause chest tightness, it's not characterized by cramping in the arm and jaw.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A rationale:
This response is dismissive of the patient's pain and does not offer any assistance. It also does not acknowledge the patient's concerns about their pain being a normal part of aging.
It's important to validate the patient's experience and offer support, even if the pain level is not severe.
This response could lead to the patient feeling unheard and unsupported, and it could potentially delay necessary treatment.
Choice B rationale:
This response suggests that the patient's pain is not significant enough to warrant treatment unless it worsens. This is not appropriate, as pain is subjective and should be treated based on the patient's individual experience.
Additionally, this response reinforces the patient's belief that pain is a normal part of aging, which may prevent them from seeking treatment in the future.
Choice C rationale:
This response is the best option because it acknowledges the patient's pain, expresses concern, and suggests further investigation.
It is important to rule out any underlying medical conditions that may be causing the pain.
This response also demonstrates to the patient that the nurse is taking their pain seriously and is committed to helping them manage it.
Choice D rationale:
This response acknowledges that pain can be a part of aging, but it also suggests that there may be a specific cause for the patient's pain.
This could lead to the patient feeling anxious or worried about their health.
It is important to investigate the cause of the pain before making any assumptions.
Correct Answer is A
Explanation
The correct answer is Choice A: Refer questions to the nursing supervisor.
Choice A rationale: By referring inquiries from other nurses to the nursing supervisor, the nurse maintains patient privacy and upholds healthcare privacy regulations, such as the Health Insurance Portability and Accountability Act (HIPAA). These regulations mandate that patient information should only be disclosed on a need-to-know basis. Referring questions to the nursing supervisor ensures that any information released is managed through the appropriate channels and protects the patient's confidentiality.
Choice B rationale: Transferring calls directly to the patient's room could infringe on their privacy and disrupt their care or rest. It is not the nurse's role to decide if the patient should be disturbed, and doing so may potentially compromise patient care and satisfaction.
Choice C rationale: Acknowledging that the person is a patient on the unit can violate confidentiality rules, as it confirms the individual's presence in the hospital and could lead to speculation about their condition. Nurses must maintain patient privacy by refraining from sharing any information, even if it seems harmless.
Choice D rationale: Contacting the patient's provider does not directly address the issue of handling inquiries from other nurses and could breach confidentiality if the provider discloses information without the patient's consent. Additionally, the provider may not be immediately available, which would delay addressing the inquiries and potentially expose the patient's privacy further.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today