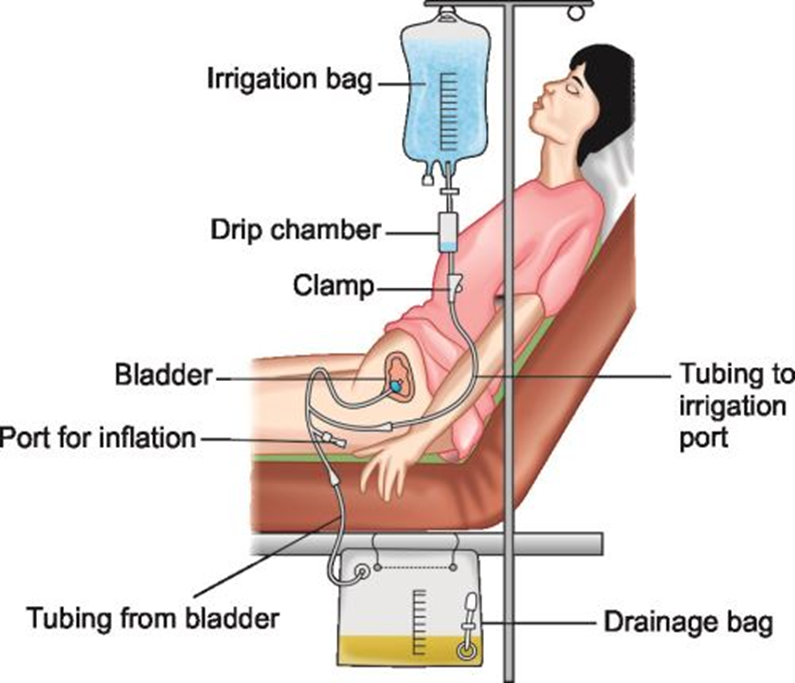
A client has an order for continuous bladder irrigation. What should the nurse do with the irrigation solution on the intake and output (I&O) sheet when calculating the fluid balance for this client?
Deduct it from the total urine output.
Subtract it from the intravenous flow sheet as output.
Document the intake hourly in the urine output column.
Add it to the oral intake column.
The Correct Answer is A
Choice A Reason:
When calculating the fluid balance for a client undergoing continuous bladder irrigation (CBI), the irrigation solution must be deducted from the total urine output. This is because the irrigation fluid is not part of the client’s actual urine production but is an additional fluid introduced into the bladder to prevent or remove blood clots and ensure catheter patency. By deducting the irrigation solution from the total urine output, the nurse can accurately determine the client’s true urine output and fluid balance.
Choice B Reason:
Subtracting the irrigation solution from the intravenous flow sheet as output is incorrect. The intravenous flow sheet is used to document fluids administered intravenously, not those introduced into the bladder. Therefore, this choice does not apply to the management of continuous bladder irrigation.
Choice C Reason:
Documenting the intake hourly in the urine output column is also incorrect. The urine output column should reflect the actual urine produced by the client, not the irrigation solution. Including the irrigation solution in this column would lead to an inaccurate representation of the client’s urine output and fluid balance.
Choice D Reason:
Adding the irrigation solution to the oral intake column is incorrect as well. The oral intake column is designated for fluids consumed orally by the client. The irrigation solution is introduced directly into the bladder and should not be recorded as oral intake.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason:
A pureed diet consists of foods that are blended to a smooth consistency. This type of diet is typically recommended for clients who have severe swallowing difficulties or are at risk of aspiration. While it can be easier to consume for those with significant dental issues, it may not provide the variety and texture that a mechanical soft diet offers, which can be more satisfying and nutritionally adequate for someone with multiple cavities and missing teeth.
Choice B Reason:
A soft diet includes foods that are easy to chew and swallow but are not necessarily blended or pureed. This diet is often recommended for clients recovering from surgery or those with mild chewing difficulties. However, for a client with multiple cavities, chipped, and missing teeth, a soft diet might still pose challenges in terms of chewing and could lead to discomfort or inadequate nutrition.
Choice C Reason:
A mechanical soft diet is specifically designed for individuals who have difficulty chewing but do not require pureed foods. This diet includes foods that are easy to chew and swallow, such as ground meats, cooked vegetables, and soft fruits. It provides a balance of texture and nutrition, making it the most appropriate choice for a client with multiple cavities, chipped, and missing teeth. This diet helps ensure the client can eat comfortably and maintain adequate nutrition.
Correct Answer is B
Explanation
Choice A Reason:
Listening to the client’s speech is not a method used to assess cranial nerve V. This method is more relevant for assessing cranial nerves IX (Glossopharyngeal) and X (Vagus), which are involved in speech and swallowing.
Choice B Reason:
Clenching the teeth is a method used to assess the motor function of cranial nerve V (the trigeminal nerve). The trigeminal nerve is responsible for the movement of the muscles involved in chewing. When a client clenches their teeth, the nurse can palpate the masseter and temporal muscles to check for strength and symmetry. This helps determine if there are any abnormalities in the motor function of the trigeminal nerve.
Choice C Reason:
Asking the client to read a Snellen chart is a method used to assess cranial nerve II (Optic), which is responsible for vision. This method does not assess cranial nerve V.
Choice D Reason:
Asking the client to raise his eyebrows is a method used to assess cranial nerve VII (Facial), which controls facial expressions. This method is not used to assess cranial nerve V.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today