A patient with respiratory failure has a respiratory rate of 26 breaths/min and an oxygen saturation (SpO2) of 80%. The patient is increasingly pale and restless but follows commands. Which intervention will the nurse anticipate?
Initiation of continuous positive pressure ventilation (CPAP)
Endotracheal intubation and positive pressure ventilation
Insertion of a mini-tracheostomy with frequent suctioning
Administration of 100% O2 by non-rebreather mask
The Correct Answer is B
B. Endotracheal intubation and positive pressure ventilation are indicated in patients with respiratory failure who are unable to maintain adequate oxygenation or ventilation with non-invasive interventions. Intubation allows for the delivery of positive pressure ventilation, oxygenation, and airway protection. It also facilitates the clearance of secretions and administration of medications. Given the patient's severe hypoxemia, impending respiratory distress, and deteriorating condition, endotracheal intubation and positive pressure ventilation are the most appropriate interventions to ensure adequate oxygenation and prevent further deterioration.
A. CPAP is a non-invasive ventilation modality that provides a continuous positive pressure to the airways throughout the respiratory cycle. While CPAP may be beneficial in certain cases of respiratory failure, it may not be sufficient for a patient with severe hypoxemia (SpO2 of 80%) and impending respiratory distress. CPAP is typically indicated for patients with conditions such as obstructive sleep apnea or mild to moderate respiratory failure.
C. Mini-tracheostomy may be considered in certain cases of upper airway obstruction or inadequate airway clearance. However, in this scenario, the patient's hypoxemia is likely due to severe respiratory failure rather than upper airway obstruction. While suctioning may be necessary to clear secretions, it does not address the underlying cause of hypoxemia or provide ventilatory support.
D. While administration of supplemental oxygen is important in the management of hypoxemia, a non- rebreather mask may not be sufficient for a patient with severe hypoxemia and impending respiratory distress. Non-rebreather masks can deliver high concentrations of oxygen but may not provide adequate positive pressure support or airway protection. In this case, endotracheal intubation and positive pressure ventilation are more appropriate to ensure adequate oxygenation and ventilation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. Positive end-expiratory pressure (PEEP) is applied during mechanical ventilation to prevent alveolar collapse at the end of expiration. It helps maintain the patency of the alveoli, improving oxygenation and preventing atelectasis.
B. While PEEP can improve oxygenation by recruiting collapsed alveoli and increasing functional residual capacity, it does not directly affect the concentration of oxygen delivered by the ventilator. Oxygen concentration is adjusted separately from PEEP settings.
C. PEEP is applied at the end of expiration to maintain positive pressure in the airways and alveoli, preventing them from collapsing. It does not directly affect the delivery of air during inhalation.
D. PEEP can help prevent lung damage by maintaining alveolar recruitment and reducing the risk of atelectasis and barotrauma. However, it is not the sole factor in preventing lung damage, and other ventilator settings and strategies also play a role in protecting the lungs.
Correct Answer is C
Explanation
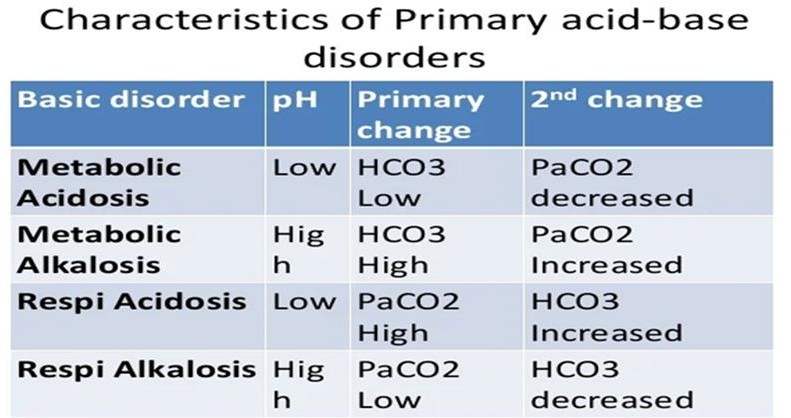
C. Respiratory acidosis- The pH is acidic, and the PaCO2 is elevated, indicating respiratory acidosis. The client's hypoventilation (respiratory rate of 7/min) is causing retention of carbon dioxide, leading to respiratory acidosis.
A. Metabolic alkalosis- The ABG values do not support a diagnosis of metabolic alkalosis. The pH is acidic, and the base excess is negative, indicating a mild metabolic acidosis.
B. Respiratory alkalosis- The ABG values do not support a diagnosis of respiratory alkalosis. The pH is acidic, and the PaCO2 is elevated, indicating respiratory acidosis rather than alkalosis.
D. Metabolic acidosis- While there is evidence of a mild metabolic acidosis indicated by the negative base excess, the primary disturbance in this case is respiratory acidosis, as evidenced by the low pH and elevated PaCO2.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today