A patient is admitted to the postpartum unit one hour after a sterile vaginal delivery of a normal neonate weighing 8 pounds 2 ounces (3.7 kg). When the client's fundus becomes boggy and displaced above the umbilicus, which action should the practical nurse (PN) take first?
Take the vital signs and open the IV infusion rate of oxytocin.
Notify the registered nurse (RN) that the client's bladder is distended.
Put the infant to breast to suckle and stimulate oxytocin secretion.
Massage the fundus and expel retained lochia and clots.
The Correct Answer is D
The practical nurse (PN) should first massage the fundus and expel retained lochia and clots to help the uterus contract and prevent postpartum hemorrhage.
Taking the vital signs and opening the IV infusion rate of oxytocin (A) may be necessary but not as urgent as massaging the fundus.
Notifying the registered nurse (RN) that the client's bladder is distended (B) is not relevant to addressing the client's boggy and displaced fundus.
Putting the infant to breast to suckle and stimulate oxytocin secretion (C) is a valid intervention, but it is not the first priority when the client's fundus becomes boggy and displaced above the umbilicus.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
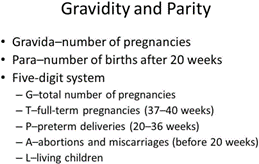
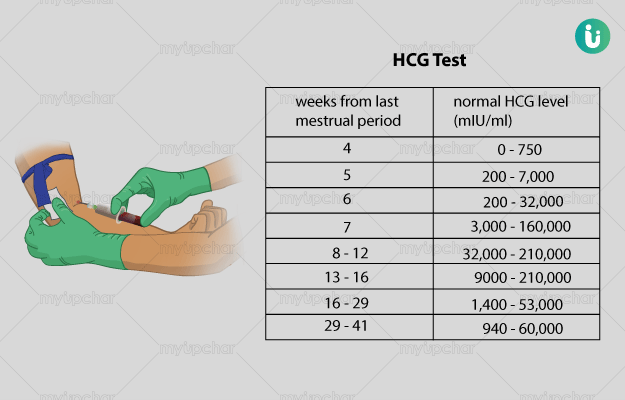
The first action the PN should take is to check the client's serum human chorionic gonadotropin (hCG) level. This hormone is produced by the placenta and can provide important information about the viability of the pregnancy.
Option B, verifying the date of the last menstrual cycle, can provide useful information about the gestational age of the pregnancy but is not the first priority.
Option C, repeating a urine pregnancy test, can confirm the presence of a pregnancy but does not provide information about its viability.
Option D, inquiring about the last occurrence of intercourse, is not relevant to addressing the client's immediate concern of vaginal bleeding.
Correct Answer is B
Explanation
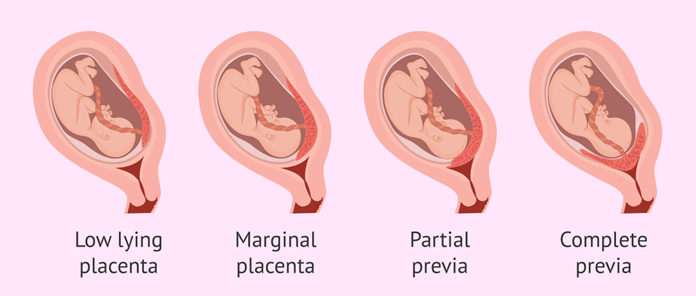
Placenta previa is a condition in which the placenta partially or completely covers the cervix, which can lead to vaginal bleeding during pregnancy. In severe cases, this bleeding can be life-threatening and can lead to hemorrhage. Therefore, the PN should closely monitor the client for any signs of bleeding or hemorrhage, such as excessive vaginal bleeding, hypotension, tachycardia, or signs of shock. The PN should also ensure that the client receives appropriate medical interventions and that emergency measures are in place in case of sudden bleeding or hemorrhage.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today