A parent asks a nurse about toys to provide for a 10-month-old infant. Which of the following toys should the nurse suggest?
Coloring book with crayons
Large-piece puzzles
Crib gym
Put-in take-out toy
The Correct Answer is C
A. Coloring book with crayons:
Coloring activities with crayons are typically more suitable for older children who have developed fine motor skills and hand-eye coordination. At 10 months old, infants are still in the early stages of motor development and may not have the dexterity to hold and manipulate crayons effectively. Additionally, infants at this age are more likely to put objects in their mouths, which poses a choking hazard with crayons.
B. Large-piece puzzles:
Puzzles with large pieces can be beneficial for older children's cognitive development by promoting problem-solving skills and hand-eye coordination. However, at 10 months old, infants are still developing their motor skills and may not have the ability to manipulate puzzle pieces effectively. Puzzles with small pieces can also pose a choking hazard for infants.
C. Crib gym:
A crib gym is a suitable toy for a 10-month-old infant as it provides opportunities for visual stimulation, reaching, grasping, and hand-eye coordination development. Crib gyms typically consist of hanging toys or objects that the infant can bat at or grasp while lying in their crib or playpen. This type of toy encourages exploration and interaction while ensuring safety within the confines of the crib.
D. Put-in take-out toy:
Put-in take-out toys involve placing objects into a container and then removing them, which can be engaging for infants. However, while this type of toy may provide some entertainment for a 10-month-old, it may not offer as much visual and tactile stimulation as a crib gym. Additionally, some put-in take-out toys may have smaller parts that pose a choking hazard for infants, so careful supervision is necessary.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A. Respiratory
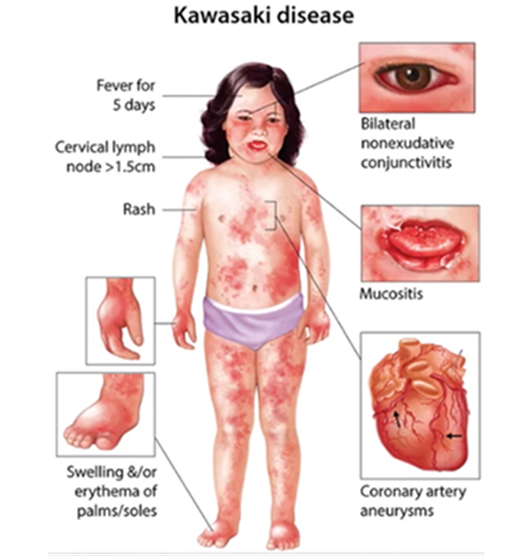
Kawasaki disease primarily affects the cardiovascular system rather than the respiratory system. While respiratory symptoms such as cough or congestion may occur in some cases, they are not the primary focus of the disease.
B. Gastrointestinal
Although gastrointestinal symptoms such as abdominal pain, vomiting, or diarrhea can occur in Kawasaki disease, they are not the primary system affected. Gastrointestinal symptoms are considered part of the systemic manifestations of the disease but do not define its primary pathology.
C. Cardiovascular
This is the correct answer. Kawasaki disease primarily affects the cardiovascular system. It is characterized by inflammation of the blood vessels, particularly the medium-sized arteries, including the coronary arteries. Coronary artery involvement can lead to coronary artery aneurysms and other cardiovascular complications, making the cardiovascular system the primary focus of the disease.
D. Integumentary
The integumentary system (skin) is not primarily affected by Kawasaki disease. While changes in the skin, such as a rash, may occur as part of the systemic manifestations of the disease, they are not the primary focus of Kawasaki disease.
Correct Answer is B
Explanation
A. Applying suction for 20 seconds:
Suctioning for 20 seconds is within the recommended duration for endotracheal suctioning in children. It allows adequate time for removing secretions without causing excessive trauma to the airway.
B. Introducing the catheter without suction:
This action is incorrect. When performing endotracheal suctioning, the catheter should be introduced into the endotracheal tube while applying suction. Introducing the catheter without suction may not effectively remove secretions and can lead to ineffective suctioning.
C. Rotating the catheter between the thumb and forefinger while suctioning:
Rotating the catheter between the thumb and forefinger while suctioning helps to prevent the catheter from sticking to the airway walls and facilitates the removal of secretions. This action is appropriate and helps ensure effective suctioning.
D. Allowing the child to rest for 30 to 60 seconds between suctioning passes:
Allowing the child to rest between suctioning passes helps minimize hypoxia and discomfort during the procedure. This action is appropriate and ensures that the child has adequate time to recover before the next suctioning pass.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today