A nurse is collecting data from a child who has spina bifida occulta. Which of the following findings should the nurse expect?
Flaccid paralysis of lower extremities
Hip dislocation
Hydrocephalus
Dimple in sacral area
The Correct Answer is D
A. Flaccid paralysis of lower extremities:
Flaccid paralysis refers to a weakness or loss of muscle tone in the affected muscles, leading to decreased or absent movement. This finding is not typically associated with spina bifida occulta. Instead, it is more commonly seen in more severe forms of spina bifida, such as myelomeningocele, where there is significant involvement of the spinal cord and nerves.
B. Hip dislocation:
Hip dislocation can occur in individuals with myelomeningocele due to muscle weakness, abnormal muscle tone, and joint deformities associated with spinal cord defects. However, it is not typically associated with spina bifida occulta, which usually presents with less severe spinal cord involvement.
C. Hydrocephalus:
Hydrocephalus, characterized by the accumulation of cerebrospinal fluid within the brain, is a common complication of myelomeningocele due to disturbances in the flow and absorption of cerebrospinal fluid caused by the spinal defect. It is less commonly associated with spina bifida occulta, which typically involves a less severe spinal cord defect.
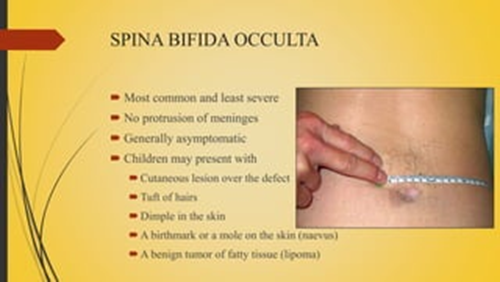
D. Dimple in sacral area:
This is the correct choice. A dimple, patch of hair, or birthmark in the lower back or sacral area is a common finding in spina bifida occulta. It occurs due to the incomplete closure of the spinal column during fetal development, leading to a small defect in the vertebrae. This is often a subtle manifestation of spina bifida occulta and may not cause significant symptoms or functional impairment.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","D"]
Explanation
A. Cranberry juice
Cranberry juice may be too acidic and could irritate the surgical site. It's best to avoid acidic beverages immediately following a tonsillectomy.
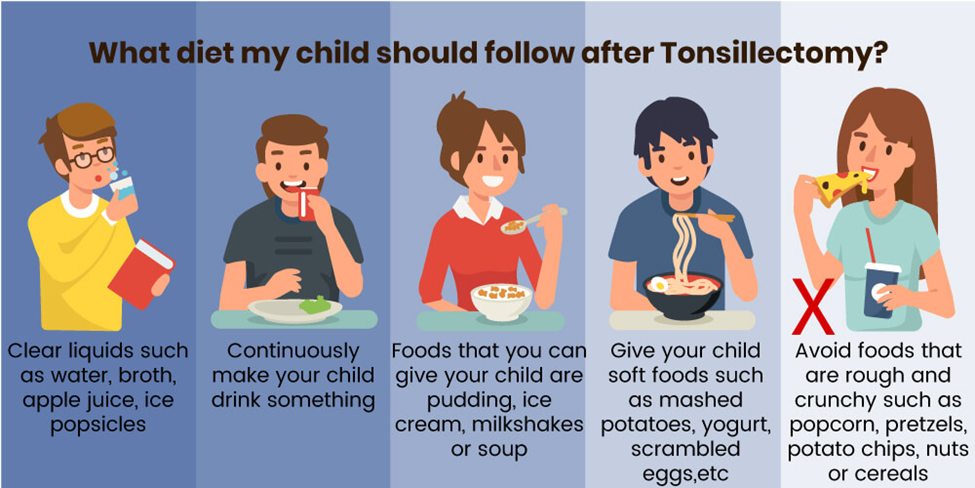
B. Ice-cream
This option is suitable. Ice-cream is cold and soothing, and it can help numb the throat, providing relief from discomfort after a tonsillectomy. However, it's essential to ensure that the ice-cream is not too cold to avoid causing discomfort.
C. Hot tea
Hot tea is not recommended immediately following a tonsillectomy. Hot liquids can irritate the surgical site and may cause discomfort. It's best to avoid hot beverages until the throat has had time to heal.
D. Italian ice
Italian ice is a frozen dessert similar to a slushy, and it can be a suitable option after a tonsillectomy. Like ice-cream, Italian ice is cold and can help numb the throat, providing relief from discomfort.
Correct Answer is A
Explanation
A. Drink eight glasses of fluid daily: This is crucial advice for patients with sickle cell anemia, as adequate hydration helps prevent sickling of red blood cells and reduces the risk of vaso-occlusive crises. Therefore, this precaution is appropriate and should be included in discharge teaching.
B. Maintain an updated Haemophilus influenzae type b (Hib) immunization: While vaccination is essential for overall health, maintaining Hib immunization is not directly related to sickle cell anemia or vaso-occlusive crises. However, it's still important for the child's general well-being and should be addressed but may not be the priority in discharge teaching for sickle cell anemia.
C. Avoid playground activities at school: Children with sickle cell anemia are at risk of vaso-occlusive crises triggered by dehydration, fatigue, or extreme physical exertion. While playground activities can be strenuous, completely avoiding them may not be necessary. Instead, the child should be educated on the importance of staying hydrated, taking breaks when needed, and avoiding excessive physical strain.
D. Assume postural drainage positions every 6 hours: Postural drainage is not typically indicated for sickle cell anemia or vaso-occlusive crises unless there are specific respiratory complications. This precaution is not relevant to the management of sickle cell anemia and should not be included in discharge teaching for this condition.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today