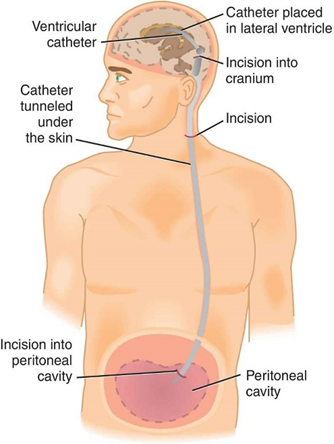
A nurse is caring for a child who is postoperative following the insertion of a ventriculoperitoneal shunt. The nurse should place the child in which of the following positions?
A 45 degree head elevation
On the nonoperative side
Prone
Supine
The Correct Answer is D
A. A 45-degree head elevation: This position can help facilitate venous drainage and reduce intracranial pressure. Elevating the head of the bed may aid in preventing the accumulation of cerebrospinal fluid (CSF) in the brain, which is important after VP shunt insertion to maintain proper drainage. However, this position alone may not be sufficient.
B. On the nonoperative side: Placing the child on the nonoperative side can help reduce pressure on the side where the shunt was inserted, minimizing discomfort and the risk of disruption or displacement of the shunt. However, this position may not directly affect CSF drainage.
C. Prone: Placing the child prone (lying face down) is generally not recommended after VP shunt insertion. This position may increase pressure on the head and interfere with proper CSF drainage, potentially leading to complications.
D. Supine: Placing the child supine (lying on their back) is typically recommended after VP shunt insertion. This position helps promote proper drainage of CSF through the shunt system without placing undue pressure on the surgical site. It also allows for easy monitoring of the child's condition and surgical site.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. Place the infant in prone position.
This option is incorrect. Placing the infant in the prone position (lying on the stomach) could put pressure on the spinal lesion, potentially causing discomfort or complications. It's important to minimize pressure on the affected area in infants with spina bifida.
B. Cover the infant's lesion with a dry cloth.
This option is incorrect. While keeping the lesion clean and dry is important for preventing infection, simply covering it with a dry cloth may not provide adequate protection. Proper wound care techniques, such as using sterile dressings and cleaning the area with prescribed solutions, are typically necessary to prevent infection and promote healing.
C. Feed the infant through an NG tube.
This option is incorrect. While infants with severe forms of spina bifida may have difficulty feeding due to associated complications, such as difficulty swallowing or weak sucking reflexes, feeding through a nasogastric (NG) tube is not a standard intervention for spina bifida itself. Feeding methods would depend on the specific needs and abilities of the infant, and may involve breastfeeding, bottle-feeding, or other methods under the guidance of healthcare professionals.
D. Diapering over a low defect will keep the infant free from infection.
This option is correct. Diapering over a low defect (the opening in the spine caused by spina bifida) helps to keep the area clean and reduce the risk of infection. By properly covering the defect with a diaper, exposure to urine and feces, which can increase the risk of infection, is minimized. Additionally, regular diaper changes and proper hygiene practices are essential for preventing complications in infants with spina bifida.
Correct Answer is ["B","C"]
Explanation
A. "You should begin to manipulate the infant's bedtime based on the hospital's visiting hours."
This statement is incorrect. Manipulating the infant's bedtime based on hospital visiting hours may disrupt the infant's regular sleep schedule, potentially causing discomfort and distress. It's important to maintain the infant's routine as much as possible to promote comfort and well-being.
B. "You should bring the infant's favorite blanket to the hospital."
This statement is correct. Bringing the infant's favorite blanket or comfort item can provide familiarity and comfort during the hospital stay. Having familiar items from home can help soothe the infant and reduce anxiety associated with the new environment.
C. "You should read the child a story about hospitalization."
This statement is correct. Reading a story about hospitalization to the child can help prepare them for the upcoming experience and alleviate fear or anxiety. Choosing age-appropriate books that explain what to expect during a hospital stay can help normalize the experience and provide reassurance to the infant and parents.
D. "You will need to go home when it is not visiting hours."
This statement is incorrect. Parents are typically allowed to stay with their infant throughout the hospitalization, especially in the case of pediatric patients. Family presence is important for providing comfort and support to the infant and facilitating bonding during the hospital stay.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today