A nurse working for a home health agency is assessing an older adult male client. Which of the following findings is the priority for the nurse to address?
Urinary hesitancy
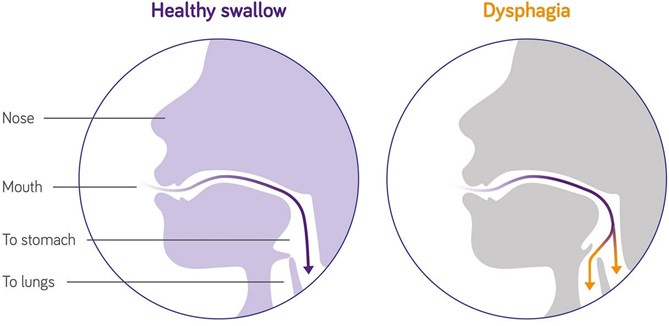
Dysphagia
Swollen gums
Pruritus
The Correct Answer is B
Choice A Reason: This choice is incorrect because urinary hesitancy is not the priority finding for the nurse to address.
Urinary hesitancy is a difficulty or delay in starting or maintaining a urine stream. It may be caused by various factors such as prostate enlargement, urinary tract infection, medication side effects, or psychological issues. It may cause discomfort, pain, or urinary retention, but it does not pose an immediate threat to the client's life.
Choice B Reason: This choice is correct because dysphagia is the priority finding for the nurse to address. Dysphagia is a difficulty or inability to swallow food or liquids. It may be caused by various factors such as stroke, Parkinson's disease, dementia, esophageal cancer, or oral infections. It may cause malnutrition, dehydration, aspiration, or choking, which can lead to serious complications such as pneumonia, sepsis, or death. Therefore, the nurse should assess the client's swallowing function and provide appropriate interventions such as modifying the diet texture, using thickening agents, or teaching swallowing techniques.
Choice C Reason: This choice is incorrect because swollen gums are not the priority finding for the nurse to address. Swollen gums are an inflammation or enlargement of the gingival tissue that surrounds the teeth. They may be caused by various factors such as poor oral hygiene, gum disease, vitamin deficiency, medication side effects, or hormonal changes. They may cause bleeding, pain, or infection, but they do not pose an immediate threat to the client's life.
Choice D Reason: This choice is incorrect because pruritus is not the priority finding for the nurse to address. Pruritus is a sensation of itching that affects the skin. It may be caused by various factors such as dry skin, allergies, eczema, psoriasis, liver disease, or kidney disease. It may cause discomfort, scratching, or skin damage, but it does not pose an immediate threat to the client's life.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: This choice is incorrect because providing a brightly lit environment may stimulate the client and increase the intracranial pressure. A brightly lit environment is an environment that has a high level of illumination or brightness. It may be used for clients who have depression, seasonal affective disorder, or insomnia, but it does not help to reduce the intracranial pressure.
Choice B Reason: This choice is incorrect because teaching controlled coughing and deep breathing may increase the intrathoracic pressure and increase the intracranial pressure. Controlled coughing and deep breathing are techniques that help to clear the airway and improve lung expansion. They may be used for clients who have respiratory infections, chronic obstructive pulmonary disease, or postoperative complications, but they do not help to reduce the intracranial pressure.
Choice C Reason: This choice is incorrect because encouraging a minimum intake of 2000 mL (67.5 oz) of clear fluids per day may cause fluid overload and increase the intracranial pressure. Fluid overload is a condition in which the body has too much fluid, which can impair the function of the heart, lungs, and kidneys. Therefore, restricting fluid intake and using diuretics may be indicated for clients who have increased intracranial pressure.
Choice D Reason: This choice is correct because elevating the head of the bed 20° may help to improve the venous drainage and decrease the intracranial pressure. As explained above, positioning the client in a semi-Fowler's or high-Fowler's position can facilitate breathing and prevent further complications. However, elevating the head of the bed more than 30° may decrease the cerebral perfusion pressure (CPP), which is the difference between the mean arterial pressure (MAP) and the intracranial pressure (ICP). A normal CPP range is 70 to 100 mm Hg, and a low CPP (<50 mm Hg) can cause cerebral ischemia, herniation, or death. Therefore, elevating the head of the bed to a moderate angle (20°) may be optimal for clients who have increased ICP.
Correct Answer is D
Explanation
Choice A: Eliciting the gag reflex is a way to assess cranial nerve IX (glossopharyngeal) and X (vagus), which are responsible for the sensation and motor function of the pharynx and larynx.
Choice B: Testing visual acuity is a way to assess cranial nerve II (optic), which is responsible for the sense of vision.
Choice C: Observing for facial symmetry is a way to assess cranial nerve VII (facial), which is responsible for the motor function of the facial muscles and the sensation of taste.
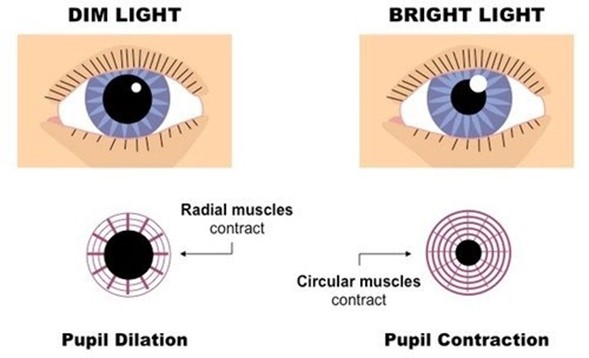
Choice D: Checking the pupillary response to light is a way to assess cranial nerve III (oculomotor), which is responsible for the motor function of most of the eye muscles, including those that control pupil size and lens shape.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today