A nurse in a critical care unit is caring for a client who suffered a knife wound to the chest. The nurse suspects the client is developing cardiac tamponade. Which of the following assessment findings should the nurse identify as supporting this suspicion?
Flatened neck veins.
Bradycardia.
Sudden lethargy.
Muffled heart sounds.
The Correct Answer is D
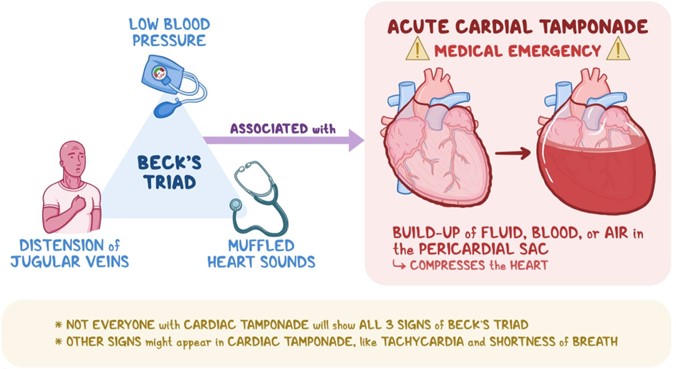
Choice A Reason: This choice is incorrect because flatened neck veins are not a sign of cardiac tamponade. Cardiac tamponade is a condition in which fluid accumulates in the pericardial sac that surrounds the heart, causing compression and impaired filling of the heart chambers. This leads to reduced cardiac output and hypotension. One of the manifestations of cardiac tamponade is distended neck veins due to increased venous pressure and impaired venous return.
Choice B Reason: This choice is incorrect because bradycardia is not a sign of cardiac tamponade. Bradycardia is a condition in which the heart rate is slower than normal (less than 60 beats per minute). It may be caused by various factors such as vagal stimulation, medication side effects, hypothyroidism, or sinus node dysfunction. It may cause symptoms such as fatigue, dizziness, or syncope, but it does not indicate cardiac tamponade.
Choice C Reason: This choice is incorrect because sudden lethargy is not a specific sign of cardiac tamponade. Lethargy is a condition in which the person feels tired, sluggish, or drowsy. It may be caused by various factors such as sleep deprivation, depression, infection, anemia, or hypoglycemia. It may affect the person's mental and physical performance, but it does not indicate cardiac tamponade.
Choice D Reason: This choice is correct because muffled heart sounds are a sign of cardiac tamponade. Muffled heart sounds are heart sounds that are fainter or softer than normal due to reduced transmission of sound waves through fluid-filled pericardial sac. They may indicate that the heart function is compromised by cardiac tamponade and require immediate intervention such as pericardiocentesis (removal of fluid from pericardial sac).
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["24"]
Explanation
- To find the concentration of heparin in the solution, divide the amount of heparin by the volume of D5W: 25,000 units / 500 mL = 50 units/mL
- To find the infusion rate, divide the prescribed dose by the concentration: 1,200 units/hr / 50 units/mL = 24 mL/hr
- Round the answer to the nearest tenth/whole number: 24 mL/hr
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because dextrose 5% in 0.9% sodium chloride is a hypertonic solution that can cause fluid overload and pulmonary edema in a client who has burns.
Choice B Reason: This is incorrect because dextrose 5% in water is a hypotonic solution that can cause fluid shifts from the intravascular space to the interstitial space, resulting in hypovolemia and hypotension in a client who has burns.
Choice C Reason: This is incorrect because 0.9% sodium chloride is an isotonic solution that can cause hypernatremia and hyperchloremia in a client who has burns, as the fluid loss from burns is greater than the sodium loss.
Choice D Reason: This is correct because lactated Ringer's is an isotonic solution that contains electrolytes similar to plasma, such as sodium, potassium, calcium, and chloride. It also contains lactate, which is converted to bicarbonate in the liver and helps correct the metabolic acidosis that occurs in a client who has burns.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today