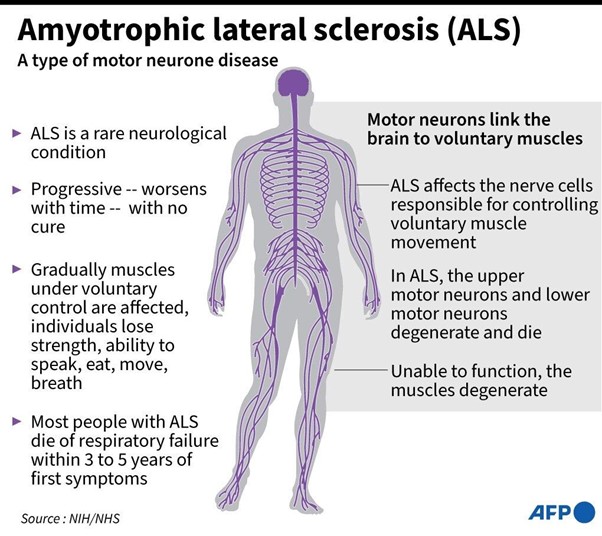
A nurse is updating the plan of care for a client who has amyotrophic lateral sclerosis with dysphagia. Which of the following interprofessional team members should the nurse identify as the priority to consult?
Dietitian
Physical therapist
Speech-language pathologist
Occupational therapist
The Correct Answer is C
Choice A option:
Dietitian should not be consulted: The dietitian is an essential team member and will work closely with the client to ensure proper nutrition and dietary management. However, in the context of dysphagia, the speech-language pathologist's expertise is needed to determine safe swallowing strategies and food modifications.
Choice B option:
Physical therapist should not be consulted: The physical therapist focuses on maintaining and improving the client's physical function and mobility. While important in ALS management, the physical therapist's role is not directly related to the immediate issue of dysphagia.
Choice C option:
The speech-language pathologist is the correct answer because it specializes in assessing and treating communication and swallowing disorders. In this case, the speech-language pathologist is essential in evaluating the client's swallowing function, recommending appropriate dietary modifications (texture and consistency of foods), and implementing swallowing exercises or strategies to improve swallowing safety.
Choice D option:
Occupational therapist should not be consulted: The occupational therapist assists clients in regaining or maintaining independence in daily living activities. While the occupational therapist may address some aspects of mealtime activities and adaptive strategies, the speech-language pathologist is more specialized in evaluating and treating swallowing difficulties in clients with ALS.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
- Urinary output is an important indicator of fluid balance and kidney function. After delivery, a woman may experience increased urinary output due to the loss of excess fluid that was retained during pregnancy and the diuretic effect of oxytocin, which is released during breastfeeding. This is a normal and expected finding in the postpartum period.
- However, increased urinary output may also be a sign of urinary retention, which is the inability to empty the bladder completely. Urinary retention can occur due to trauma to the bladder or urethra during delivery, swelling or hematoma of the perineum, epidural anesthesia, or decreased bladder sensation.Urinary retention can lead to complications such as infection, bladder distension, or postpartum hemorrhage.
- Therefore, when a woman who delivered a normal newborn 24 hours ago reports that she seems to be urinating every hour or so, the practical nurse (PN) should measure the next voiding, then palpate the client's bladder. This will help to assess the amount and quality of urine and the presence or absence of bladder distension. A normal urine output is about 30 ml per hour, and a normal bladder should feel soft and empty after voiding. If the urine output is low or high, or if the bladder feels firm or full after voiding, the PN should report these findings to the primary healthcare provider for further evaluation and intervention.
Therefore, option B is the correct answer, while options A, C, and D are incorrect.
Option A is incorrect because catheterizing the client for residual urine volume is an invasive procedure that should only be done if indicated by the primary healthcare provider.
Option C is incorrect because evaluating for normal involution and massaging the fundus are related to uterine function, not urinary function.
Option D is incorrect because obtaining a specimen for urine culture and sensitivity is not necessary unless there are signs of infection, such as fever, dysuria, or foul-smelling urine.
Correct Answer is A
Explanation
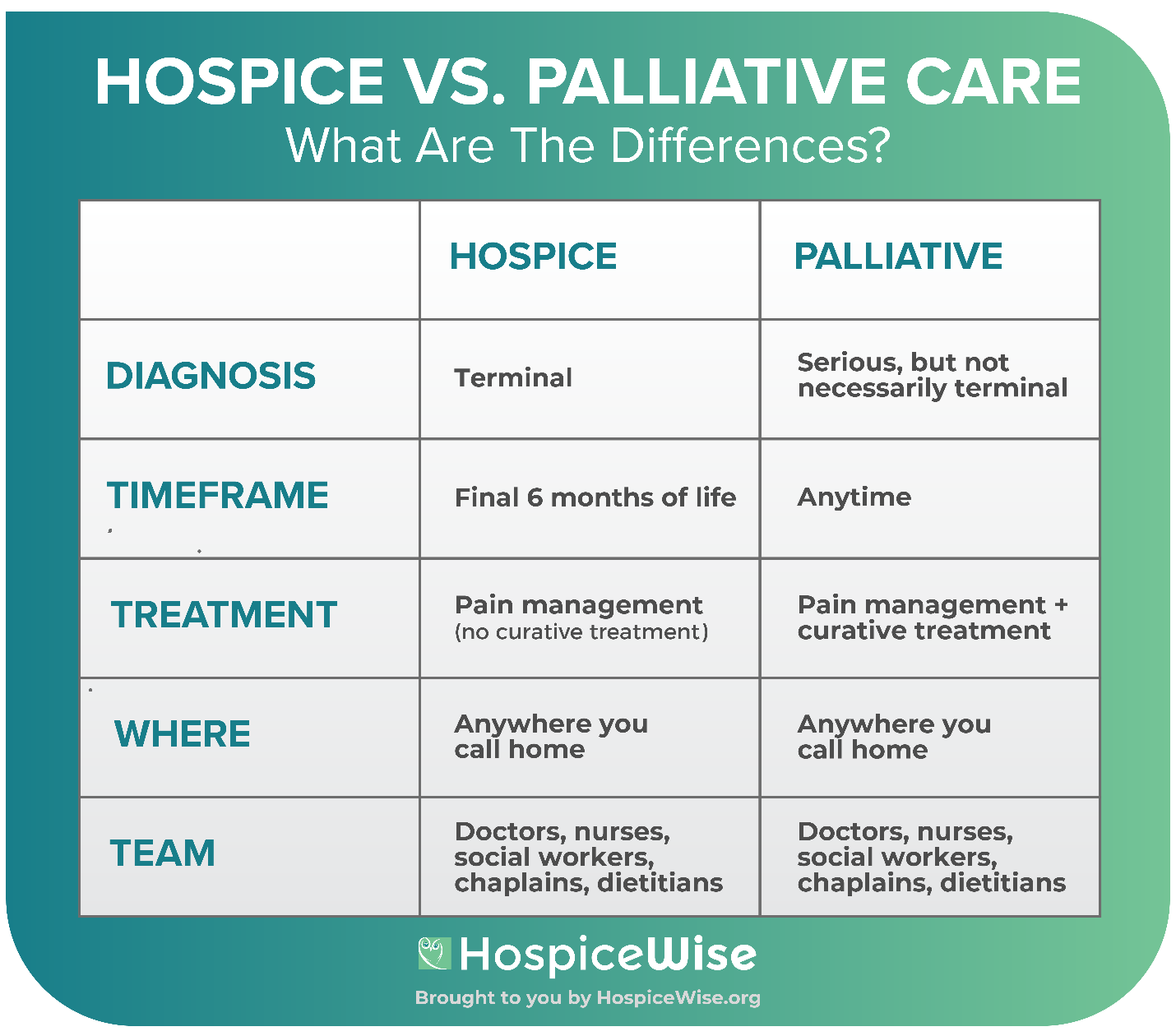
A is correct because hospice care includes bereavement support for the family for up to a year after the client's death.
B is incorrect because the hospice nurse does not administer pain medication, but rather teaches the family how to manage the client's pain at home.
C is incorrect because respite care is one of the services that hospice provides to allow the family to take a break from caregiving.
D is incorrect because hospice care does not aim to prolong life, but rather to provide comfort and quality of life for the client and the family.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today