A nurse is planning care for a client who has rheumatoid arthritis. Which of the following interventions should the nurse include in the plan?
Encourage the client to take a cool sponge bath each morning.
Administer opioid analgesia.
Increase the client's dietary iron intake.
Restrict the client's intake of foods high in purines.
The Correct Answer is C
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Heart rate 136/min is a normal finding for a newborn. The normal range of heart rate for a newborn is 100 to 160/min.
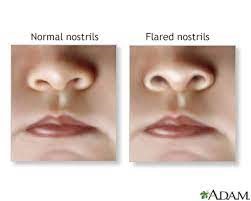
B. Nasal flaring is an abnormal finding for a newborn. Nasal flaring indicates respiratory distress and may be caused by conditions such as pneumonia, meconium aspiration, or congenital heart defects.
C. Transient strabismus is a normal finding for a newborn. Transient strabismus is a temporary misalignment of the eyes that occurs due to weak eye muscles and poor coordination. It usually resolves by 3 to 6 months of age.
D. Overlapping of sutures is a normal finding for a newborn. Overlapping of sutures is caused by molding of the skull during delivery and allows the head to fit through the birth canal. It usually resolves within a few days after birth.
Correct Answer is B
Explanation
A. Incorrect. Performing gastrostomy feedings is a complex task that requires specialized training and assessment skills. The nurse should not delegate this task to an AP who has not received the appropriate education and competency validation.
B. Correct. Determining if the PRN pain medication has helped is a simple task that involves asking the client about their pain level and documenting the response. The nurse can delegate this task to an AP as long as they follow up with the client and evaluate the effectiveness of the pain management plan.
C. Incorrect. Providing instructions about client care to a family member over the telephone is a task that requires clinical judgment and communication skills. The nurse should not delegate this task to an AP who might not have the knowledge or authority to answer questions or address concerns.
D. Incorrect. Teaching a client how to measure their own blood pressure is a task that requires teaching and evaluation skills. The nurse should not delegate this task to an AP who might not be able to explain the procedure, demonstrate the technique, or assess the client's learning.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today