A nurse is caring for a client who had abdominal surgery 24 hr ago. Which of the following actions is the nurse's priority?
Assess fluid intake every 24 hr.
Ambulate three times a day.
Assist with deep breathing and coughing.
Monitor the incision site for findings of infection.
The Correct Answer is C
A. Assessing fluid intake every 24 hr is important for a postoperative client, but it is not the priority action. The nurse should monitor fluid intake and output more frequently, such as every 8 hr or every shift, to detect any imbalances or complications.
B. Ambulating three times a day is beneficial for a postoperative client, but it is not the priority action. The nurse should encourage early and frequent ambulation to promote circulation, prevent thromboembolism, and enhance bowel function, but only after ensuring that the client is stable and has adequate pain control.
C. Assisting with deep breathing and coughing is the priority action for a postoperative client who had abdominal surgery. The nurse should help the client perform these exercises every 1 to 2 hr to prevent atelectasis, pneumonia, and respiratory failure, which are common and serious complications after abdominal surgery.
D. Monitoring the incision site for findings of infection is important for a postoperative client, but it is not the priority action. The nurse should inspect the wound for signs of infection, such as redness, swelling, warmth, drainage, or odor, but this can be done during routine dressing changes or as needed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
a. Administer the medication and alert the charge nurse: This choice suggests proceeding with medication administration but also informing the charge nurse. While it's important to communicate with the charge nurse regarding medication administration, in this scenario, there is no indication to hold the medication as the infant's heart rate is within the normal range. Therefore, alerting the charge nurse may not be necessary at this point.
b. Hold the medication and document cardiac assessment: This choice suggests holding the medication and documenting the cardiac assessment. However, since the infant's heart rate is within the normal range for their age, there is no clinical indication to hold the medication. Holding the medication unnecessarily could delay treatment and potentially lead to adverse outcomes if the medication is needed.
c. Administer the medication and document the heart rate.
Since the infant's heart rate of 120 beats per minute falls within the normal range for a 2-month-old, there is no indication to hold the medication. Administering the digoxin as prescribed and documenting the heart rate before administration are appropriate actions. It's important to ensure accurate documentation to track the infant's response to the medication and monitor for any changes in heart rate.
d. Hold the medication and recheck the heart rate in 1 hour: This choice suggests holding the medication and rechecking the heart rate in 1 hour. Again, since the infant's heart rate is within the normal range, there is no clinical indication to hold the medication or delay treatment. Rechecking the heart rate in 1 hour would be unnecessary and could potentially delay necessary medication administration.
Correct Answer is A
Explanation
- Seizure precautions are measures taken to protect a client who is at risk of having a seizure, which is a sudden and abnormal electrical activity in the brain that can cause changes in behavior, movement, sensation, or consciousness. Seizure precautions include providing a safe environment, monitoring the client's vital signs and neurological status, administering anticonvulsant medications, and documenting the onset, duration, and characteristics of any seizure activity.
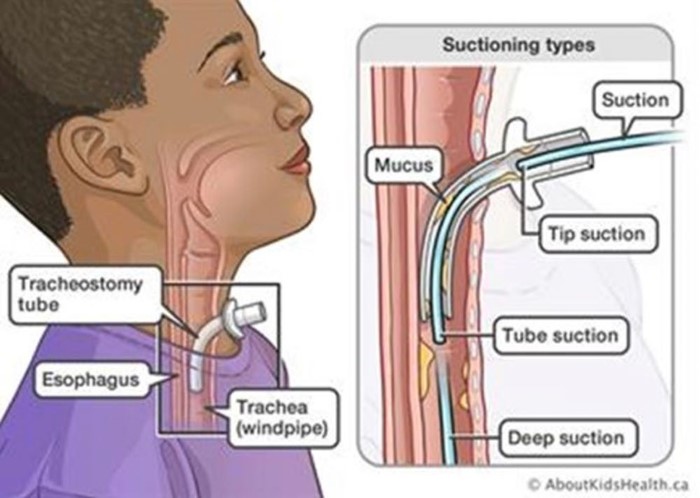
- One of the potential complications of a seizure is aspiration, which is the inhalation of foreign material into the lungs, such as saliva, vomit, or food. Aspiration can cause choking, pneumonia, or respiratory distress. To prevent or treat aspiration, the practical nurse (PN) should ensure the ready availability of equipment to perform suctioning of the trachea, which is the tube that connects the mouth and nose to the lungs. Suctioning of the trachea involves inserting a catheter through the nose or mouth into the trachea and applying negative pressure to remove any secretions or debris from the airway.
- Therefore, option A is the correct answer, while options B, C, and D are incorrect.
Option B is incorrect because inserting a urinary catheter is not related to seizure precautions or aspiration prevention.
Option C is incorrect because applying soft restraints may not be necessary or appropriate for a client who requires seizure precautions, as they may interfere with the natural movements of the seizure or cause injury to the client.
Option D is incorrect because inserting a nasogastric tube is not related to seizure precautions or aspiration prevention.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today