A nurse is teaching a group of clients about risk factors for developing diabetes mellitus. The nurse should include which of the following as a risk factor for diabetes?
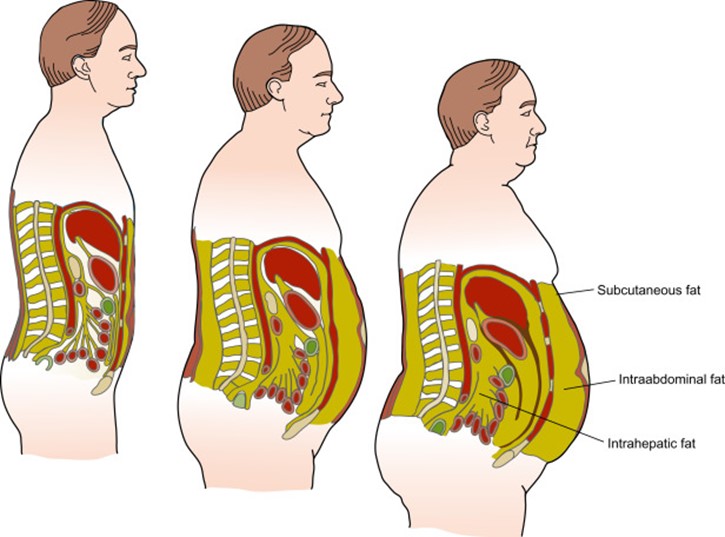
Abdominal obesity
Elevated HDL level
History of hypotension
History of hyperthyroidism
The Correct Answer is A
Choice A reason: Abdominal obesity is a risk factor for developing diabetes mellitus. Abdominal obesity, also known as central obesity or visceral fat, is the accumulation of fat around the abdomen and organs. Abdominal obesity can cause insulin resistance, inflammation, and metabolic syndrome, which are all associated with diabetes.
Choice B reason: Elevated HDL level is not a risk factor for developing diabetes mellitus. HDL stands for high-density lipoprotein, which is a type of cholesterol that carries excess cholesterol from the tissues to the liver for disposal. HDL is also known as "good" cholesterol, as it helps protect against heart disease and stroke. A high HDL level is desirable and beneficial for health.
Choice C reason: History of hypotension is not a risk factor for developing diabetes mellitus. Hypotension means low blood pressure, which is usually defined as less than 90/60 mm Hg. Hypotension can cause symptoms such as dizziness, fainting, fatigue, and blurred vision. Hypotension can be caused by dehydration, blood loss, medication side effects, or other conditions.
Choice D reason: History of hyperthyroidism is not a risk factor for developing diabetes mellitus. Hyperthyroidism means overactive thyroid gland, which produces too much thyroid hormone. Thyroid hormone regulates metabolism, growth, and development. Hyperthyroidism can cause symptoms such as weight loss, nervousness, palpitations, heat intolerance, and insomnia. Hyperthyroidism can be caused by Graves' disease, thyroid nodules, or thyroiditis.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: Dry eyes are not caused by vitamin D deficiency, but by other factors such as aging, medication, environmental conditions, or eye diseases. Vitamin D does not have a direct role in eye health or function.
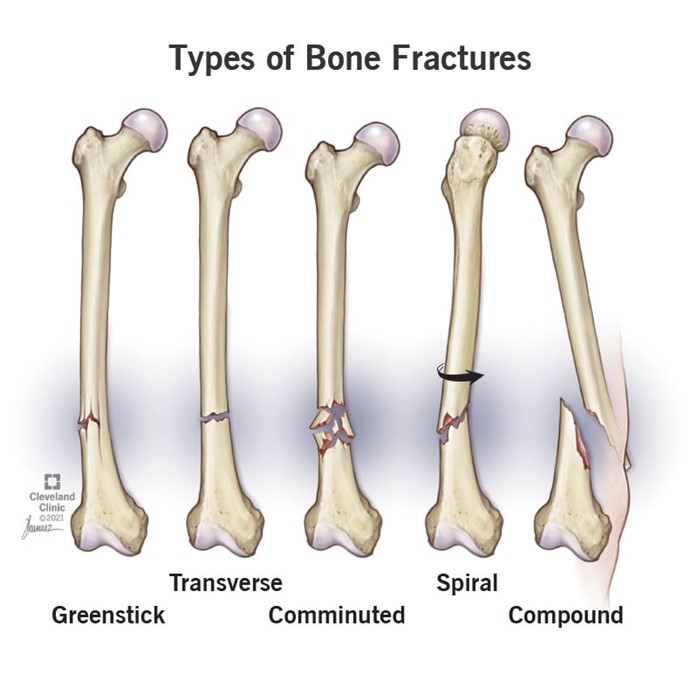
Choice B reason: Fractures are caused by vitamin D deficiency, as vitamin D helps the body absorb calcium, which is essential for bone health and strength. Vitamin D deficiency can lead to osteoporosis, a condition in which the bones become brittle and prone to breaking.
Choice C reason: Infection is not caused by vitamin D deficiency, but by other factors such as exposure to pathogens, weakened immune system, or poor hygiene. Vitamin D may have some role in modulating immune responses, but it is not a primary factor in preventing infection.
Choice D reason: Swelling is not caused by vitamin D deficiency, but by other factors such as injury, inflammation, fluid retention, or allergic reaction. Vitamin D does not have a direct role in regulating fluid balance or reducing inflammation.
Correct Answer is C
Explanation
Choice A reason: Using an electronic device is not a reliable method for measuring blood pressure because it may give inaccurate readings due to movement, noise, or battery issues. An electronic device should be calibrated regularly and compared with a manual device.
Choice B reason: Inflating the cuff to 140/90 mmHg is not a correct procedure for measuring blood pressure because it may cause discomfort and false readings. The cuff should be inflated to about 20 to 30 mmHg above the expected systolic pressure or until the pulse disappears.
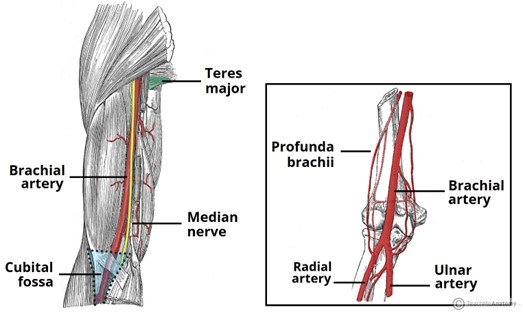
Choice C reason: Placing the cuff on the upper arm is a correct procedure for measuring blood pressure because it ensures that the cuff is at the same level as the heart and that the brachial artery is compressed. The cuff should be snug and fit around 80% of the arm circumference.
Choice D reason: Measuring blood pressure after exercise is not a good time for measuring blood pressure because it may reflect a temporary increase due to physical activity. Blood pressure should be measured after resting for at least 5 minutes in a quiet and comfortable environment.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today