A nurse is preparing to review discharge instructions with a client who reports having hearing loss. Which of the following actions should the nurse plan to take?
Stand next to the client when speaking.
Guide the client away from background noise.
Provide a copy of the instructions printed in Braille.
Repeat any phrases that the client misunderstands.
Correct Answer : A,B,D
Choice A Reason: This is a correct choice. Standing next to the client when speaking is an action that the nurse should plan to take, as it helps the client hear better and see the nurse's facial expressions and lip movements. The nurse should also speak clearly and slowly, use simple words and sentences, and avoid covering their mouth.
Choice B Reason: This is a correct choice. Guiding the client away from background noise is an action that the nurse should plan to take, as it reduces distractions and interference with hearing. The nurse should also choose a well-lit and quiet place for communication and turn off any unnecessary devices or appliances.
Choice C Reason: This is an incorrect choice. Providing a copy of the instructions printed in Braille is not an action that the nurse should plan to take, as it is not helpful for clients with hearing loss. Braille is a system of raised dots that represents letters and numbers for people who are blind or visually impaired. The nurse should provide a copy of the instructions printed in large font or use pictures or diagrams to supplement verbal information.
Choice D Reason: This is a correct choice. Repeating any phrases that the client misunderstands is an action that the nurse should plan to take, as it ensures comprehension and clarification of important information. The nurse should also ask open-ended questions, encourage feedback, and summarize key points at the end of the conversation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: The burned area is yellow in color with severe edema is not a finding of a deep partial-thickness burn, but a superficial partial-thickness burn. A superficial partial-thickness burn involves the epidermis and the upper layer of the dermis, causing pain, redness, swelling, and blistering.
Choice B Reason: The burned area is black in color and pain is absent is not a finding of a deep partial-thickness burn, but a full-thickness burn. A full-thickness burn involves the epidermis, dermis, and underlying tissues, causing necrosis, charred skin, and loss of sensation.
Choice C Reason:This description aligns with a superficial partial-thickness (first-degree or mild second-degree) burn rather than a deep partial-thickness burn. Superficial partial-thickness burns involve the epidermis and the upper portion of the dermis. These burns appear pink or red, often accompanied by moisture and blister formation due to fluid leakage from damaged capillaries. They are painful because nerve endings remain intact. Healing occurs within 10 to 21 days without significant scarring.
Choice D Reason:Deep partial-thickness burns extend deeper into the dermis, damaging a larger portion of skin structures, including sweat glands and hair follicles. These burns typically appear red or white and may have a soft eschar (dead tissue), which differentiates them from more superficial burns that do not develop eschar. Unlike full-thickness burns, nerve endings remain partially intact, so the patient may still experience some pain. These burns take more than 21 days to heal and often require skin grafting to prevent complications such as contractures or hypertrophic scarring.
Correct Answer is A
Explanation
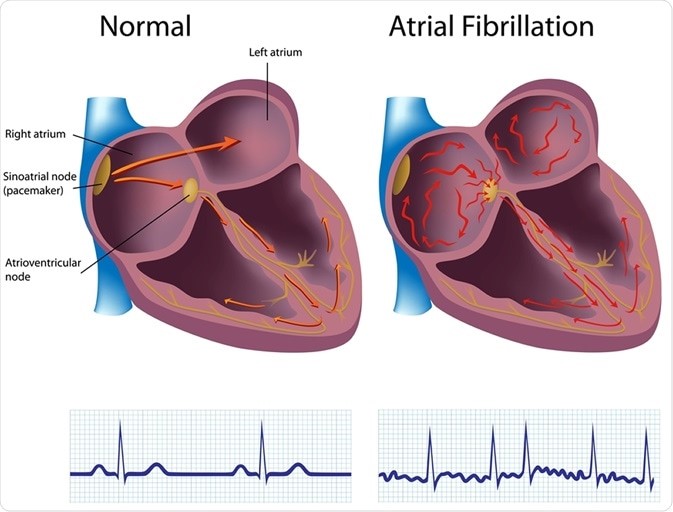
Choice A reason: This is the correct answer because atrial fibrillation is the risk factor that puts the client at
the highest risk for embolic stroke. Atrial fibrillation is an irregular and rapid heart rate that causes poor blood flow and blood pooling in the heart chambers. This can lead to the formation of blood clots that can travel to the brain and block an artery, causing an embolic stroke.
Choice B reason: This is incorrect because hypertension is not the risk factor that puts the client at
the highest risk for embolic stroke. Hypertension is high blood pressure that puts stress on the blood vessels and increases the risk of bleeding or rupture. This can lead to a hemorrhagic stroke, but not an embolic stroke.
Choice C reason: This is incorrect because diabetes is not the risk factor that puts the client at
the highest risk for embolic stroke. Diabetes is a condition that causes high blood sugar levels and damages the blood vessels and nerves. This can lead to poor circulation and increased risk of infection and ulcers, but not an embolic stroke.
Choice D reason: This is incorrect because alcohol abuse is not the risk factor that puts the client at
the highest risk for embolic stroke. Alcohol abuse is excessive consumption of alcohol that affects liver function and blood clotting factors. This can lead to liver disease and bleeding disorders, but not an embolic stroke.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today