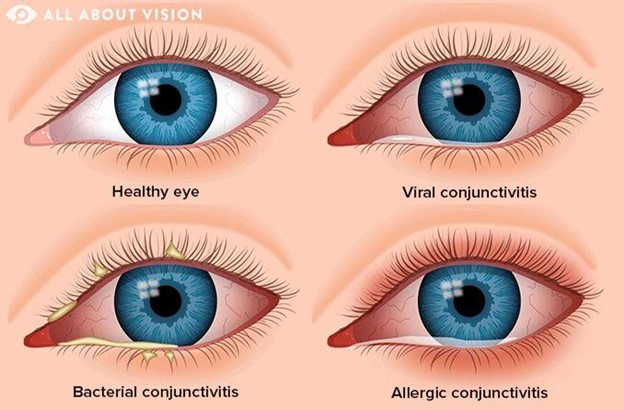
A client arrives with a pink eye that is itchy, swollen, and uncomfortable with a creamy discharge. Which of the following home care instructions will the nurse offer to the client?
Wash towels, sheets, and pillowcases
Use antifungal drops 3 times a day
Schedule a sexually transmitted infection (STI/STD) exam
Avoid going outside during daylight hours
The Correct Answer is A
Choice A Reason: This is the correct choice. Washing towels, sheets, and pillowcases is a home care instruction that the nurse will offer to the client, as it prevents reinfection and transmission of bacteria or viruses. The client has conjunctivitis, which is inflammation of the conjunctiva or thin membrane that covers the white part of the eye and lines the eyelids. It can be caused by bacteria, viruses, allergies, or irritants.
Choice B Reason: This is an incorrect choice. Using antifungal drops 3 times a day is not a home care instruction that the nurse will offer to the client, as it is not effective for conjunctivitis. Antifungal drops are used for fungal infections of the eye, which are rare and usually occur after trauma or surgery. The client may need antibiotic or antiviral drops, depending on the cause of conjunctivitis.
Choice C Reason: This is an incorrect choice. Scheduling a sexually transmitted infection (STI/STD) exam is not a home care instruction that the nurse will offer to the client, as it is not relevant for conjunctivitis. STIs can affect the eyes, but they usually cause different symptoms, such as redness, pain, or discharge from the urethra or vagina. The client may need to be tested for STIs if they have other risk factors or signs of infection.
Choice D Reason: This is an incorrect choice. Avoiding going outside during daylight hours is not a home care instruction that the nurse will offer to the client, as it is not necessary for conjunctivitis. The client may experience sensitivity to light, but they can wear sunglasses or avoid direct sunlight to protect their eyes. The client should also avoid rubbing or touching their eyes, wear glasses instead of contact lenses, and discard any eye makeup or cosmetics that may be contaminated.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
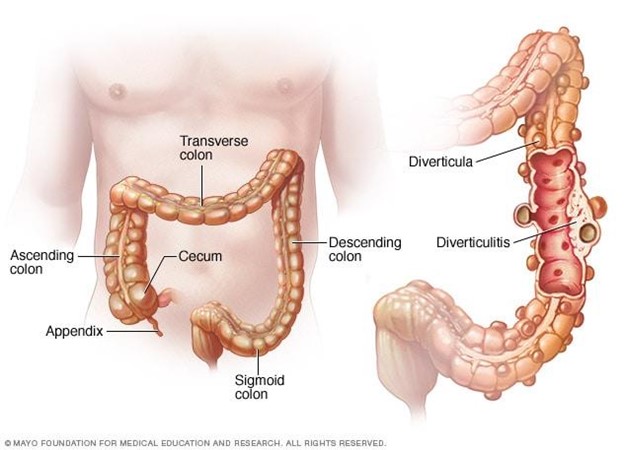
Choice A Reason: Increasing protein from red meat is not part of client education, as it can worsen the condition and increase the risk of complications. Red meat is high in fat and low in fiber, which can cause constipation and increase the pressure in the colon. Diverticulosis is a condition where small pouches or sacs form in the wall of the colon due to weak spots or increased pressure.
Choice B Reason: Decreasing fluid intake is not part of client education, as it can worsen the condition and increase the risk of complications. Fluid intake should be increased to prevent dehydration and promote bowel movements. Diverticulosis can cause abdominal pain, bloating, cramping, and changes in bowel habits.
Choice C Reason: Incorporating soft foods that are pureed in consistency is not part of client education, as it can worsen the condition and increase the risk of complications. Soft foods are low in fiber and can cause constipation and increase the pressure in the colon. Diverticulosis can lead to diverticulitis, which is inflammation or infection of the pouches or sacs.
Choice D Reason: This is the correct choice. Increasing dietary fiber is part of client education, as it can improve the condition and prevent complications. Fiber helps soften the stool and reduce the pressure in the colon. Diverticulosis can be managed by eating a high-fiber diet, drinking plenty of fluids, exercising regularly, and avoiding straining or holding stools.
Correct Answer is A
Explanation
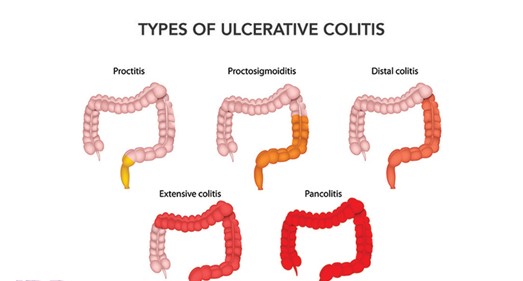
Choice A reason: This is the correct answer because both ulcerative colitis and Crohn's disease are inflammatory bowel diseases (IBD) that cause chronic inflammation of the digestive tract. The inflammation can cause symptoms such as abdominal pain, diarrhea, bleeding, weight loss, or fever. The nurse should educate the client on how to manage inflammation and prevent complications.
Choice B reason: This is incorrect because both ulcerative colitis and Crohn's disease do not affect the entire alimentary canal, but different parts of it. Ulcerative colitis affects only the colon (large intestine) and rectum, while Crohn's disease can affect any part of the digestive tract from mouth to anus, most commonly the ileum (the last part of the small intestine). The nurse should explain the differences in location and extent of
the diseases.
Choice C reason: This is incorrect because both ulcerative colitis and Crohn's disease do not always require a bowel diversion, but only in some cases. A bowel diversion is a surgical procedure that creates an opening (stoma) in the abdomen to divert fecal matter into an external bag or pouch. It may be done to treat severe complications such as perforation, obstruction, fistula, or cancer. The nurse should inform the client about the indications, types, and care of bowel diversions.
Choice D reason: This is incorrect because both ulcerative colitis and Crohn's disease are not caused by low-fat, high-fiber diets, but by unknown factors. The exact causes of IBD are not clear, but they may involve genetic, immune, environmental, or microbial factors. Low-fat, high-fiber diets may help prevent or reduce symptoms of IBD, but they do not cause them. The nurse should advise the client on how to follow a balanced and nutritious diet that suits their individual needs and preferences.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today