A nurse is planning care for an 8-month-old infant who has heart failure. Which of the following actions should the nurse include in the plan of care?
Administer cool, humidified oxygen via nasal cannula.
Place the infant in a prone position.
Repeat a digoxin dosage if the infant vomits within 1 hr of administration.
Provide less frequent, higher volume feedings.
The Correct Answer is A
Infants with heart failure often present with breathing trouble1, and administering oxygen can help improve oxygen delivery.
Choice B is wrong because placing an infant in a prone position does not help with heart failure.
Choice C is wrong because if an infant vomits within 1 hour of administration of digoxin, the dosage should not be repeated without consulting a healthcare provider.
Choice D is wrong because infants with heart failure may have feeding issues and providing less frequent, higher volume feedings may not be helpful34.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Provide for periods of rest.
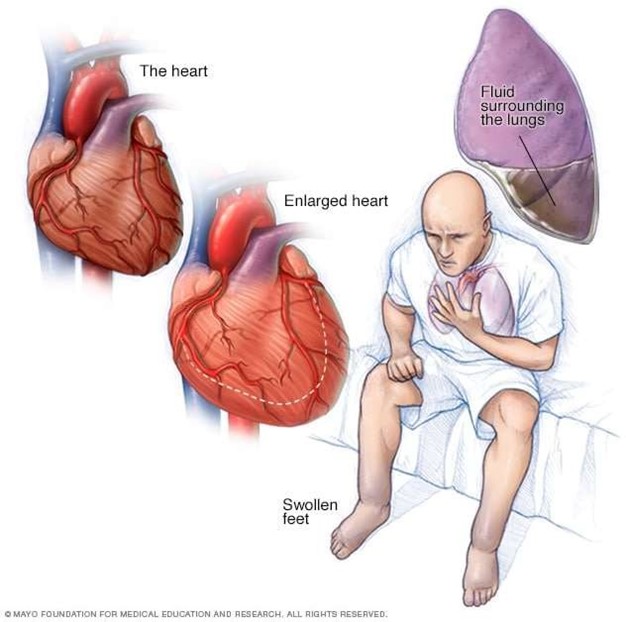
Children with heart failure may have trouble breathing, especially with activity, and may feel tired.
It is important for them to have periods of rest to help manage their symptoms.
Choice A is wrong because increasing the child’s oxygen flow rate should be done under the guidance of a healthcare provider.
Choice B is wrong because it is important to monitor the child’s weight more frequently than once a month.
Choice C is wrong because digoxin is a medication that can help the heart beat stronger with a more regular rhythm and should not be withheld based on pulse rate alone.
Correct Answer is A
Explanation
The nurse should request verbal consent from the client for STI testing.
All 50 states and the District of Columbia explicitly allow minors to consent for their own STI services.
Choice B is wrong because it is not necessary to contact the client’s parents to obtain phone consent.
Choice C is wrong because it is not necessary to postpone the testing until the client’s parents are present.
Choice D is wrong because written consent is not required for STI testing.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today