A nurse is performing an assessment of a newborn's Babinski reflex. Which of the following findings should the nurse expect?
Flexion of the forearm.
Downward curl of the toes.
Dorsiflexion of the great toe.
Extension of the leg.
The Correct Answer is C
The Babinski reflex, also known as the plantar reflex, is a normal reflex in infants
that occurs when the sole of the foot is stroked from heel to toe.
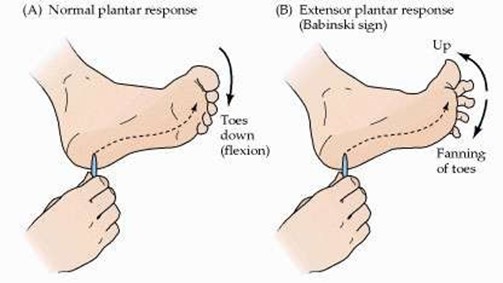
In response to this stimulus, the big toe moves upward or toward the top surface of the foot and the other toes fan out.
Choice A is not an answer because flexion of the forearm is not a response to stimulation of the foot.
Choice B is not an answer because downward curl of the toes is not a response
to stimulation of the foot.
Choice D is not an answer because extension of the leg is not a response to
stimulation of the foot.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","E"]
Explanation
The nurse should plan to immunize the client with the inactivated influenza vaccine (A) and the diphtheria-acellular pertussis vaccine (E).

The Centers for Disease Control and Prevention (CDC) recommends that pregnant women get two vaccines during every pregnancy: the inactivated flu vaccine and the Tdap vaccine.
The other vaccines listed are not recommended during pregnancy:
- The human papillomavirus vaccine is not recommended during pregnancy.
- The varicella vaccine is not recommended during pregnancy.
- The measles, mumps, and rubella vaccine is not recommended during pregnancy.
Correct Answer is D
Explanation
Do not retract the foreskin to clean your baby’s penis during each diaper change.
The foreskin should not be retracted for cleaning during infancy.

Choice A is incorrect because you should clean around the umbilical cord stump with plain water and blot dry until it falls off naturally.
Choice B is incorrect because swaddling a baby tightly with their legs extended is not recommended.
Choice C is incorrect because a newborn should urinate at least six times a day.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today