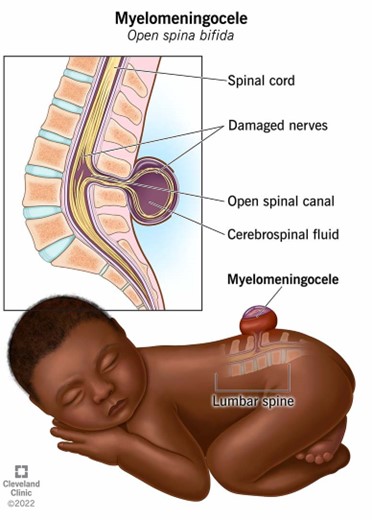
A nurse is orienting a newly licensed nurse in the care of an infant who has myelomeningocele.
Which of the following actions by the new nurse indicates the teaching has been effective?
Takes an axillary temperature.
Places the infant in a side-lying position.
Maintains a dry dressing over the sac.
Performs range of motion on the infant's hips.
The Correct Answer is A
A. Infants with spina bifida, including those with myelomeningocele, have an increased risk of rectal anomalies, so avoiding rectal temperatures is essential. The correct and safe method of temperature measurement for these infants is typically axillary.
B. Placing the infant in a side-lying position is not recommended for a child with myelomeningocele. The preferred position is prone to avoid pressure on the sac and reduce the risk of rupture and infection.
C. Maintains a dry dressing over the sac: While the sac should be kept covered, it is typically kept moist with sterile saline-soaked gauze to prevent it from drying out and to minimize the risk of infection.
D. Performs range of motion on the infant's hips: Range of motion exercises might be indicated later on, but initially, the focus is on protecting the sac and preventing complications.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The nurse should first offer the mother's private time with the newborn to allow her to grieve and say goodbye.
This can be an important part of the healing process for the mother.
Choice A is not an answer because contacting clergy is not the first action the nurse should take.
Choice B is not an answer because transferring the client to another unit is not the first action the nurse should take.
Choice C is not an answer because administering medication is not the first action the nurse should take.
Correct Answer is B
Explanation
A cerebral palsy is a group of disorders that affect movement and muscle tone or posture.
It’s caused by damage that occurs to the immature, developing brain, most often before birth.
Signs and symptoms appear during infancy or preschool years.
In general, cerebral palsy causes impaired movement associated with exaggerated reflexes, floppiness or spasticity of the limbs and trunk, unusual posture, involuntary movements, unsteady walking, or some combination of these.
An 8-month-old infant with cerebral palsy may have developmental delays and may require pillow props to sit up.
Choice A, Tracking an object with eyes, is a normal developmental milestone for
an infant.
Choice C, Uses a pincer grasp to pick up a toy, is also a normal developmental
milestone for an infant.
Choice D, Smiles when a parent appears, is also a normal developmental milestone for an infant.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today