A nurse is obtaining a health history from a client who has diverticular disease. Which of the following should the nurse identify as a risk factor for this condition?
Low dietary intake of fiber
Prolonged use of steroids
Insufficient intake of protein
Family history of gallbladder disease
The Correct Answer is A
Choice A rationale:
Low dietary intake of fiber is a significant risk factor for diverticular disease. A diet low in fiber can lead to constipation and increased pressure in the colon, contributing to the formation of diverticula.
Choice B rationale:
Prolonged use of steroids is not a primary risk factor for diverticular disease.
Choice C rationale:
Insufficient intake of protein is not a significant risk factor for diverticular disease.
Choice D rationale:
Family history of gallbladder disease is not directly associated with an increased risk of diverticular disease.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A rationale:
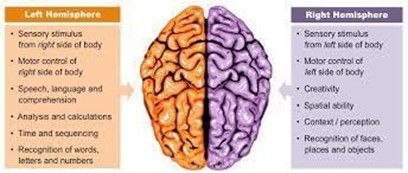
Aphasia, or difficulty with language, is more commonly associated with left hemispheric stroke.
Choice B rationale:
Depression can be a common psychological reaction following stroke, but it is not a specific finding associated with right hemispheric stroke.
Choice C rationale:
Right hemispheric stroke can lead to loss of depth perception and spatial awareness due to its impact on the visual-spatial processing areas of the brain.
Choice D rationale:
Slow, cautious behavior is a common finding after stroke regardless of the affected hemisphere.
Correct Answer is A
Explanation
Choice A rationale:
Tachycardia (rapid heart rate) is a common early indicator of excessive blood loss. It is the body's compensatory response to decrease in circulating blood volume.
Choice B rationale:
Flushed skin is not necessarily indicative of excessive blood loss. Pallor may be more characteristic.
Choice C rationale:
Polyuria (increased urine output) is not a reliable indicator of blood loss and is not commonly associated with postpartum hemorrhage.
Choice D rationale:
A firm fundus is a positive sign and indicates the uterus is contracting appropriately. It is not indicative of excessive blood loss.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today