A nurse is contributing to the plan of care for a client 48 hr following cesarean birth. Which of the following nonpharmacologic interventions should the nurse include to reduce pain from intestinal gas?
Provide the client with a carbonated beverage.
Encourage the client to lie on their right side.
Encourage the client to ambulate.
Provide the client with straws for beverages.
The Correct Answer is A
Choice A reason:
The nurse should provide the client with a carbonated beverage as a nonpharmacologic intervention to reduce pain from intestinal gas. Carbonated beverages, like soda or sparkling water, can help alleviate gas by promoting burping, which releases trapped gas from the digestive system. The effervescence of the carbonated drink can help relieve the discomfort caused by accumulated gas, offering relief to the client.
Choice B reason:
Encouraging the client to lie on their right side is not an effective nonpharmacologic intervention for reducing pain from intestinal gas. Although positioning can sometimes aid in relieving discomfort, lying on the right side does not specifically target the reduction of gas. Therefore, it is not the most appropriate choice in this scenario.
Choice C reason:
Encouraging the client to ambulate is a beneficial nonpharmacologic intervention for various post-operative conditions. However, when it comes to reducing pain from intestinal gas, it may not be as effective as other options. While movement can aid in gas passage through the digestive system, it might not be the most immediate or direct solution for alleviating the client's discomfort.
Choice D reason:
Providing the client with straws for beverages does not directly address the issue of intestinal gas. It is an unrelated intervention and may not provide any significant relief for the client's discomfort.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason:
The nurse should not remind the client to void every 4 hours because epidural anesthesia can cause temporary loss of bladder sensation, making it difficult for the client to know when to void. Instead, the nurse should use a bladder scanner to assess for urinary retention and encourage the client to void regularly.
Choice B reason:
Encouraging the client to alternate from side to side every 2 hours is not directly related to the administration of epidural anesthesia. This action is commonly advised for clients who are on bed rest to prevent pressure ulcers and promote circulation. However, it is not specifically necessary for the client receiving epidural anesthesia for pain management during labor.
Choice C reason:
Raising the four side rails on the client's bed is not necessary in this situation. The use of side rails should be based on the client's mobility and risk assessment for falls. If the client is receiving epidural anesthesia, they may experience reduced mobility, but the decision to use side rails should be made on an individual basis, not solely based on the anesthesia.
Choice D reason:
Monitoring the client's blood pressure is a crucial action when a client is receiving epidural anesthesia. Epidural anesthesia can cause a drop in blood pressure, leading to hypotension. By regularly monitoring the client's blood pressure, the nurse can detect any significant changes and take appropriate actions to maintain hemodynamic stability.
Correct Answer is B
Explanation
Choice A reason:
One cup of oatmeal - Oatmeal is a nutritious food, but it does not contain as high a protein content as some other options. While it offers some protein, it is not the best choice for a high-protein diet during pregnancy. Oatmeal is primarily known for its fiber content and complex carbohydrates, which provide sustained energy.
Choice B reason:
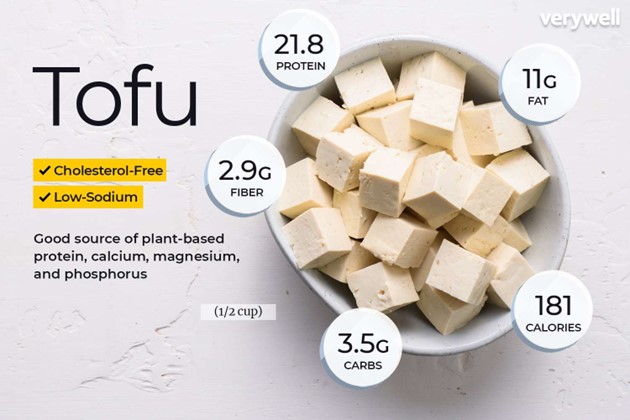 One cup of tofu - Tofu is an excellent source of protein and is a suitable choice for a high- protein diet during pregnancy. Tofu is made from soybeans and is rich in plant-based proteins, making it an ideal option for individuals following a vegetarian or vegan diet as well. Additionally, tofu contains essential amino acids, iron, calcium, and other nutrients beneficial for both the mother and the developing fetus.
One cup of tofu - Tofu is an excellent source of protein and is a suitable choice for a high- protein diet during pregnancy. Tofu is made from soybeans and is rich in plant-based proteins, making it an ideal option for individuals following a vegetarian or vegan diet as well. Additionally, tofu contains essential amino acids, iron, calcium, and other nutrients beneficial for both the mother and the developing fetus.
Choice C reason:
One cup of brown rice - While brown rice is a healthy whole grain and provides some protein, it does not have as high a protein content as tofu. Brown rice is a good source of complex carbohydrates, fiber, vitamins, and minerals, but it may not meet the high protein requirements of a pregnant woman's diet.
Choice D reason:
One cup of kale - Kale is a nutritious leafy green vegetable, but it does not offer a significant amount of protein compared to tofu. It is rich in vitamins, minerals, and antioxidants, making it a valuable addition to a balanced diet. However, for a high-protein diet during pregnancy, other options like tofu are more suitable.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today