A nurse is reinforcing teaching with a client who is postpartum and plans to breastfeed their newborn. Which of the following statements by the client indicates an understanding of the teaching?
"I should add 500 calories per day to my diet.”
"I will use antibacterial soap and warm water to wash my breasts.”
"Breastfeeding is a reliable method of birth control.”
"If my nipples become cracked and red, I will apply hydrocortisone cream.”
The Correct Answer is B
Choice A reason:
The client stating, "I should add 500 calories per day to my diet,” is not an accurate understanding of breastfeeding. While it is true that breastfeeding mothers require additional calories to support lactation, the specific amount of calories needed varies depending on individual factors and should be discussed with a healthcare professional. Simply adding 500 calories per day may not be appropriate for every woman and could lead to excessive weight gain.
Choice B reason:
This choice indicates an understanding of proper breast hygiene during breastfeeding. Using antibacterial soap and warm water to wash the breasts helps to prevent infection and maintain good breast health, reducing the risk of complications for both the mother and the baby.
Choice C reason:
The statement, "Breastfeeding is a reliable method of birth control,” is incorrect. While breastfeeding can provide some natural contraceptive effects, it is not a foolproof method of birth control. This concept is known as the lactational amenorrhea method (LAM), and specific criteria must be met for it to be considered a reliable form of contraception. Relying solely on breastfeeding as birth control can lead to an unintended pregnancy.
Choice D reason:
The statement, "If my nipples become cracked and red, I will apply hydrocortisone cream,” is not advisable. While hydrocortisone cream may provide temporary relief from irritation, it is not recommended for breastfeeding mothers. Ingestion of the cream by the baby can be harmful. Instead, the client should seek guidance from a healthcare professional to address and resolve any breastfeeding-related nipple issues.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason:
Airborne precautions are implemented for diseases that spread through small airborne particles, such as tuberculosis or measles. These diseases can remain suspended in the air for extended periods and be inhaled by others. Pertussis, also known as whooping cough, is primarily spread through respiratory droplets when an infected person coughs or sneezes, making airborne precautions unnecessary.
Choice B reason:
Droplet precautions are appropriate for illnesses that spread through respiratory droplets produced when an infected person talks, coughs, or sneezes. Pertussis falls into this category as it is transmitted mainly through respiratory droplets. By implementing droplet precautions, the nurse will minimize the risk of transmission to others, including healthcare workers and other patients.
Choice C reason:
Standard precautions are the baseline infection prevention practices used for all patients to prevent the spread of infections in healthcare settings. While important, they may not be sufficient to control the transmission of pertussis, as it requires additional measures like droplet precautions due to its specific mode of transmission.
Choice D reason:
Neutropenic precautions are used for patients with compromised immune systems, particularly those with low white blood cell counts (neutropenia). The purpose is to protect these vulnerable individuals from exposure to infectious agents. However, pertussis precautions are different and do not fall under the neutropenic category.
Correct Answer is B
Explanation
Choice A reason:
The nurse should prioritize Choice B over Choice A as it is essential to first confirm the correct placement of the NG tube before proceeding with any other actions. If the tube is not correctly positioned, administering the enteral feeding can lead to potential complications, such as aspiration, which can be life-threatening. Therefore, it is crucial to ensure the NG tube's proper placement before moving forward with the feeding
Choice B reason:
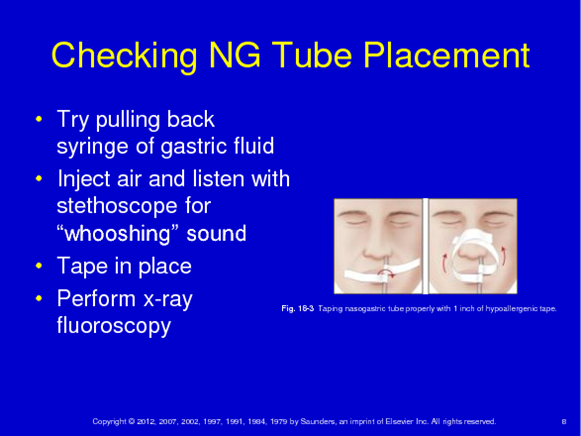
This option takes precedence as verifying the NG tube's position is a fundamental step in the enteral feeding process. The nurse must use appropriate methods, such as X-ray or pH testing, to confirm that the tube is in the stomach and not in the respiratory tract or elsewhere. This verification ensures the safety and effectiveness of the feeding procedure and prevents potential harm to the child.
Choice C reason:
While checking the gastric residual volume (GRV) is an important step in some cases, it should be done after confirming the NG tube's proper placement (Choice B). GRV provides information about the amount of feeding left in the stomach and helps in assessing tolerance to the feeding. However, if the NG tube is misplaced, determining GRV becomes irrelevant as the feeding would not be going to the intended location.
Choice D reason:
Flushing the child's NG tube with sterile water is an appropriate step during the enteral feeding process but should be done after verifying the tube's position (Choice B). Flushing ensures that the tube is patent and free from any obstructions, allowing the feeding to pass through smoothly. However, again, if the NG tube is incorrectly positioned, flushing it would not address the underlying issue.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today