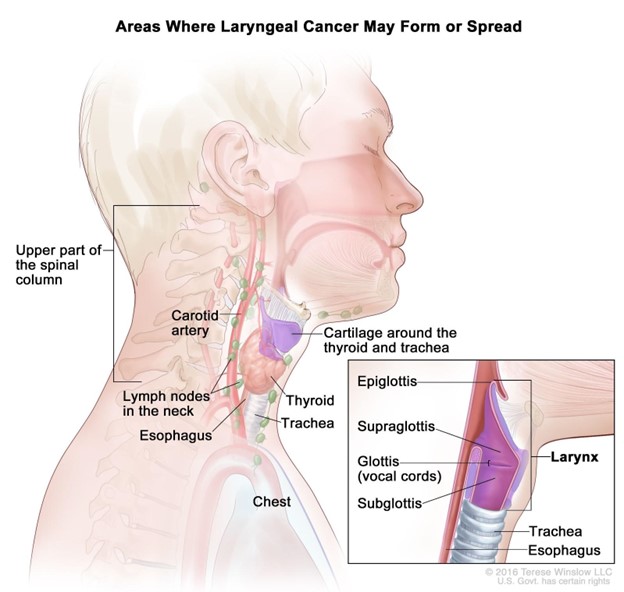
A nurse is collecting data from a client diagnosed with laryngeal cancer who is postoperative following a laryngectomy. Which of the following is a clinical manifestation of a hemorrhage?
Increased pain
Continuous swallowing
Poor fluid intake
Drooling
The Correct Answer is B
Choice A Reason: Increased pain is not a specific sign of hemorrhage, but it may indicate inflammation, infection, or nerve damage.
Choice B Reason: Continuous swallowing is a sign of hemorrhage, as it indicates that blood is accumulating in the throat or esophagus and stimulating the swallowing reflex.
Choice C Reason: Poor fluid intake is not a sign of hemorrhage, but it may indicate difficulty swallowing, nausea, or dehydration.
Choice D Reason: Drooling is not a sign of hemorrhage, but it may indicate impaired oral control, salivary gland damage, or infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A Reason: Keeping scissors at the bedside is the most important safety intervention for this client, as it allows for quick removal of the tube in case of airway obstruction or bleeding.
Choice B Reason: Providing good mouth care is an important intervention for this client, but it is not the most important, as it helps to prevent oral infections and discomfort.
Choice C Reason: Deflating the balloon on a regular basis is not an appropriate intervention for this client, as it may cause bleeding or displacement of the tube.
Choice D Reason: Monitoring IV fluid intake is an important intervention for this client, but it is not the most important, as it helps to prevent fluid overload or dehydration.
Correct Answer is ["A","B","C"]
Explanation
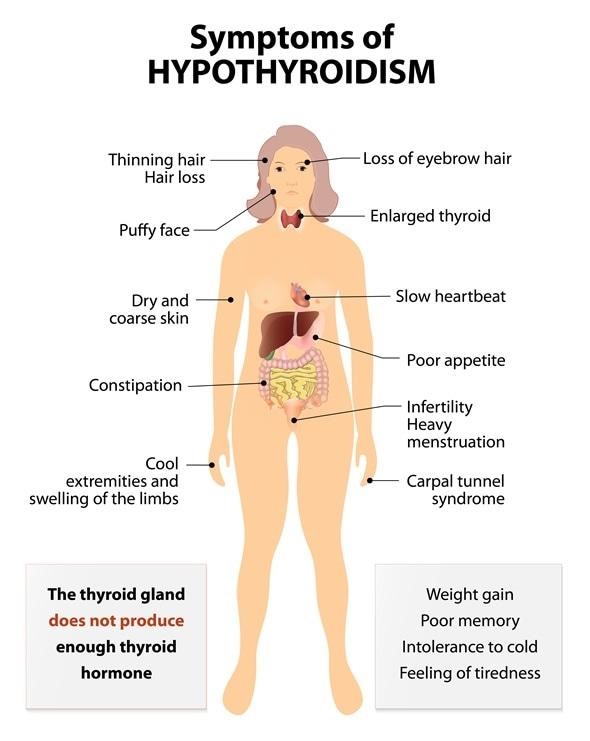
Choice A Reason: Heat intolerance is a common finding in hyperthyroidism, as the increased metabolic rate causes the body to produce more heat and sweat.
Choice B Reason: Diarrhea is a common finding in hyperthyroidism, as the increased motility of the gastrointestinal tract causes more frequent and loose stools.
Choice C Reason: Weight loss is a common finding in hyperthyroidism, as the increased metabolism and appetite cause the body to burn more calories than it consumes.
Choice D Reason: Weight gain is not a common finding in hyperthyroidism, but it may indicate other conditions such as hypothyroidism or Cushing's syndrome.
Choice E Reason: Bradycardia is not a common finding in hyperthyroidism, but it may indicate other conditions such as heart block or beta-blocker use.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today