A client admitted to a medical-surgical unit for surgery has a history of Cushing's syndrome. Which physical assessment finding would the nurse expect to observe?
Buffalo hump and moon face
Dry, scaly skin and cold intolerance
Dry, sticky mucous membranes and hypovolemia
Exophthalmos and tachycardia
The Correct Answer is A
Choice A Reason: Buffalo hump and moon face are physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, as they indicate fat redistribution and accumulation due to excess cortisol production.
Choice B Reason: Dry, scaly skin and cold intolerance are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hypothyroidism, which affects the metabolism and skin condition.
Choice C Reason: Dry, sticky mucous membranes and hypovolemia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate dehydration or diabetes insipidus, which affect the fluid balance and urine output.
Choice D Reason: Exophthalmos and tachycardia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hyperthyroidism, which affects the eye protrusion and heart rate.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: N0 does not indicate presence of regional lymph node involvement, but absence of it. N1 to N3 indicate increasing degrees of regional lymph node involvement.
Choice B Reason: TIS does not indicate that a tumor has been resolved, but that it is in situ, meaning that it is confined to the original site and has not invaded deeper tissues.
Choice C Reason: T4 does not indicate a tumor at its smallest size, but at its largest size. T1 to T4 indicate increasing sizes or extents of the primary tumor.
Choice D Reason: M1 indicates tumor metastasis to a single site, meaning that the cancer has spread to another organ or distant lymph node. M0 indicates no distant metastasis.
Correct Answer is D
Explanation
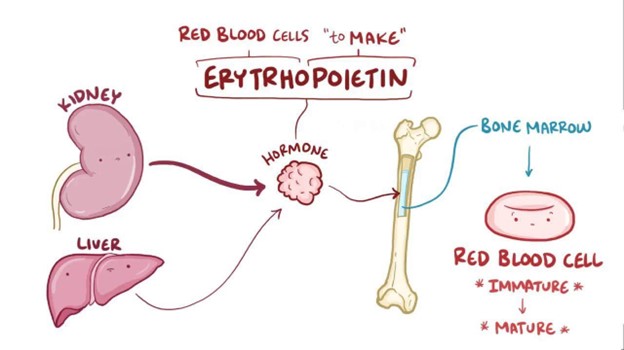
Choice A Reason: Loss of erythropoietin will not result in diminished immunologic function, but it may affect the production of some white blood cells and antibodies.
Choice B Reason: Loss of erythropoietin will not result in hypertension, but it may cause hypotension due to reduced blood volume and viscosity.
Choice C Reason: Loss of erythropoietin will not result in elevated lipid levels in the bloodstream, but it may be associated with dyslipidemia due to other factors such as malnutrition, inflammation, or medication use.
Choice D Reason: Loss of erythropoietin will result in anemia, as erythropoietin is a hormone that stimulates the bone marrow to produce red blood cells.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today