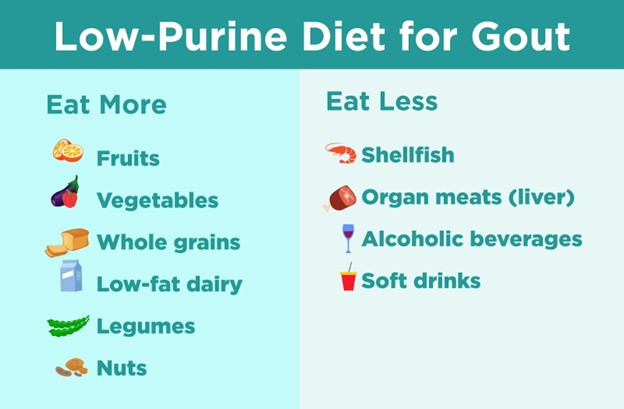
A nurse is reinforcing teaching for a client about following a low-purine diet to manage gout. Which of the following statements should the nurse identify as an indication that the client understands the instructions?
I'll drink white wine, not red.
I'll limit the number of fruit servings I eat each day.
I'll avoid eating organ meats.
I'll choose red meat instead of poultry.
The Correct Answer is C
Choice A Reason: Drinking white wine, not red, is not an indication that the client understands the instructions, as both types of wine are high in purine and may trigger gout attacks.
Choice B Reason: Limiting the number of fruit servings I eat each day is not an indication that the client understands the instructions, as most fruits are low in purine and may help to lower uric acid levels.
Choice C Reason: Avoiding eating organ meats is an indication that the client understands the instructions, as organ meats are very high in purine and may increase uric acid levels and cause gout flare-ups.
Choice D Reason: Choosing red meat instead of poultry is not an indication that the client understands the instructions, as both red meat and poultry are high in purine and may worsen gout symptoms.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: Assisting the RN to prepare an IV insulin infusion is not the first action that the nurse should take, as it may not be appropriate for the client's condition without knowing the blood glucose level.
Choice B Reason: Giving the client 4 oz of orange juice is not the first action that the nurse should take, as it may worsen the client's condition if the blood glucose level is high.
Choice C Reason: Checking the client's capillary blood glucose is the first action that the nurse should take, as it helps to determine if the client has hyperglycemia or hypoglycemia and guides the appropriate intervention.
Choice D Reason: Assisting the RN to administer 50% dextrose is not the first action that the nurse should take, as it may be harmful for the client if the blood glucose level is high.
Correct Answer is B
Explanation
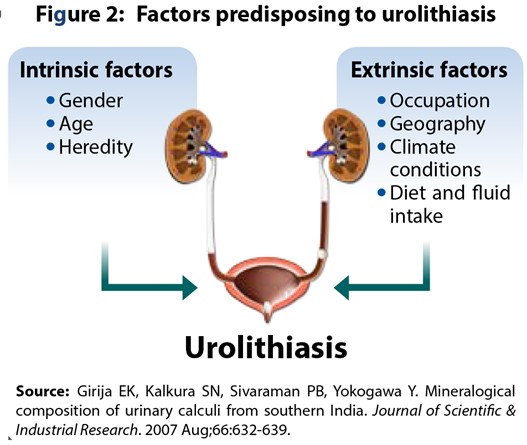
Choice A Reason: Telling the client to expect a decrease in urine output is not an appropriate intervention for a client who has urolithiasis, as it may indicate dehydration, obstruction, or infection.
Choice B Reason: Encouraging the client to drink 3 L of fluids per day is an appropriate intervention for a client who has urolithiasis, as it helps to flush out stones, prevent new stone formation, and reduce urinary concentration.
Choice C Reason: Providing the client with a high protein diet is not an appropriate intervention for a client who has urolithiasis, as it may increase uric acid and calcium excretion and promote stone formation.
Choice D Reason: Maintaining the client on bed rest is not an appropriate intervention for a client who has urolithiasis, as it may decrease renal perfusion and increase urinary stasis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today