A nurse is caring for a client who complains that he feels as though his ear is blocked and tells the nurse that he has a history of cerumen impaction in the external ear. The nurse, inspecting the ears for cerumen impaction, checks for which finding?
The presence of edema in the external auditory canal
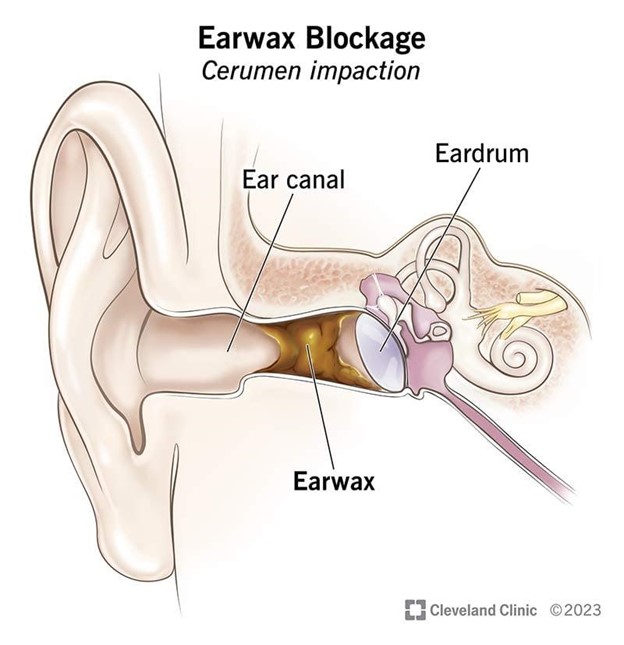
A yellowish or brownish waxy material in the external auditory canal
Redness and swelling of the tympanic membrane
An external auditory canal that is longer than normal
The Correct Answer is B
Choice A Reason: The presence of edema in the external auditory canal is not a sign of cerumen impaction, but it may indicate other conditions such as otitis externa or allergic reaction.
Choice B Reason: A yellowish or brownish waxy material in the external auditory canal is a sign of cerumen impaction, as it shows that there is excess or hardened earwax that blocks the ear canal.
Choice C Reason: Redness and swelling of the tympanic membrane are not signs of cerumen impaction, but they may indicate other conditions such as otitis media or trauma.
Choice D Reason: An external auditory canal that is longer than normal is not a sign of cerumen impaction, but it may be a normal variation or a result of aging.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: Telling the client that this is to be expected after surgery is not the first action that the nurse should take, as it may indicate a complication such as increased intraocular pressure, hemorrhage, or infection.
Choice B Reason: Placing the client in a supine position is not the first action that the nurse should take, as it may worsen the pain and increase intraocular pressure.
Choice C Reason: Documenting the findings is not the first action that the nurse should take, as it may delay the intervention and outcome.
Choice D Reason: Notifying the surgeon is the first action that the nurse should take, as it indicates that the client needs immediate evaluation and treatment to prevent vision loss or permanent damage to the eye.
Correct Answer is ["A","C","E"]
Explanation
Choice A Reason: History of alcohol abuse is an additional information that the nurse should obtain from this client, as it may indicate liver damage or cirrhosis, which can cause clay-colored stool due to reduced bile production or flow.
Choice B Reason: Intolerance to fatty foods is not an additional information that the nurse should obtain from this client, as it does not relate to clay-colored stool, but it may indicate gallbladder disease or malabsorption.
Choice C Reason: Pain in the RUQ radiating to the shoulder is an additional information that the nurse should obtain from this client, as it may indicate gallstone obstruction or inflammation, which can cause clay-colored stool due to blocked bile ducts.
Choice D Reason: Pain in the McBurney's point is not an additional information that the nurse should obtain from this client, as it does not relate to clay-colored stool, but it may indicate appendicitis or diverticulitis.
Choice E Reason: Bleeding ulcer is an additional information that the nurse should obtain from this client, as it may indicate upper gastrointestinal bleeding, which can cause clay-colored stool due to digested blood.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today