A nurse is collecting data for a client who is receiving enteral tube feedings. The nurse should identify that which of the following findings is a manifestation of fluid overload?
Weight loss
Decreased blood pressure
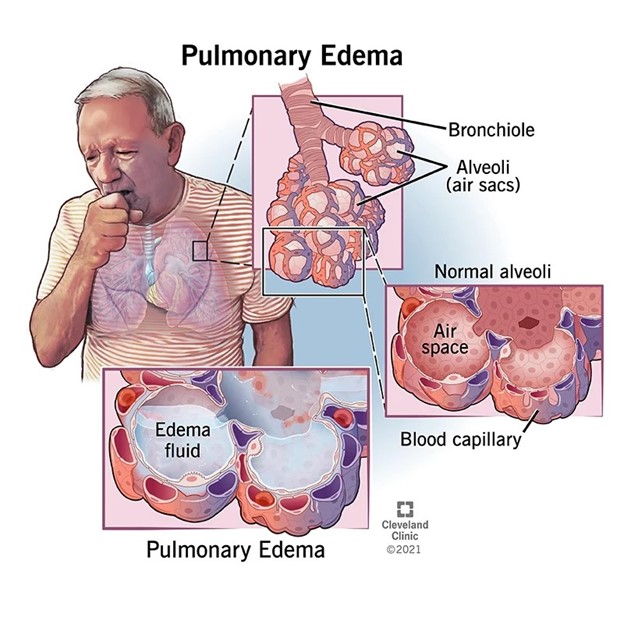
Crackles heard in the lungs
Decreased skin turgor
The Correct Answer is C
Fluid overload refers to an excess volume of fluid in the body, which can occur as a result of various factors, including excessive fluid intake or inadequate fluid removal. Crackles heard in the lungs, also known as rales, can indicate fluid accumulation in the lungs, a condition known as pulmonary edema. It is a common manifestation of fluid overload and can be detected through auscultation of the lungs.
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
Weight loss is typically associated with inadequate calorie or nutrient intake, rather than fluid overload.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Dependent personality disorder is characterized by an excessive reliance on others for decision-making and a fear of being alone or taking responsibility. Encouraging the client to be assertive helps promote their independence and self-confidence. It allows them to express their needs and preferences, make decisions, and take responsibility for their own actions. Empowering the client to be assertive can enhance their overall well-being and promote healthier relationships.
Limiting the client's social interactions may exacerbate their dependency and hinder their progress in developing more self-reliance and independent coping skills. It is important to encourage appropriate and healthy social interactions while also promoting the client's independence.
Maintaining a verbal no-harm contract with the client is a strategy more commonly used for clients at risk of self-harm or harm to others. It may not be directly applicable to the care of a client with dependent personality disorder unless there are specific safety concerns. Assuming responsibility for making the client's decisions would reinforce their dependency and enable their avoidance of taking personal responsibility. It is important to promote autonomy and support the client in making their own decisions whenever possible.
Correct Answer is B
Explanation
Before any invasive procedure, it is essential to ensure that the client has given informed consent. Informed consent involves providing the client with detailed information about the procedure, its risks and benefits, and alternatives. The client should have the opportunity to ask questions and fully understand the procedure before giving consent.
Oral contrast solutions are typically used for imaging procedures such as CT scans or X-rays, not for esophagogastroduodenoscopy. This procedure involves the insertion of a flexible tube with a camera into the esophagus, stomach, and duodenum to visualize the upper gastrointestinal tract.
While it is important to provide the client with information about the duration of the procedure, stating a specific time frame may not be accurate or helpful. The duration of an esophagogastroduodenoscopy can vary depending on factors such as the complexity of the procedure and the client's individual circumstances.
Having a full bladder is not necessary for an esophagogastroduodenoscopy procedure. This requirement may be relevant for other procedures, such as pelvic ultrasound, but it is not applicable in this case.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today