A nurse is assisting with the care of a client. Laboratory Results
1100:
Abdominal ultrasound: mass present in small intestine proximal to ileocecal valve. Size of mass is 6 cm x 7 cm (2.4 in x 2.8 in).
Select the 4 responsibilities the nurse has in relation to the client's advance directives.
Provide the client with written information about advance directives
Instruct the client that an advance directive is a legal document and must be honored by care providers
Initiate a power of attorney for health care document
Communicate advance directives status via the medical record and shift report
Document that the provider discussed-do-not-resuscitate status with the client
Inform the client that an advance directive discontinues further care
Correct Answer : A,B,C,D
Provide the client with written information about advance directives: It is important for the nurse to educate the client about advance directives, their purpose, and how they can make informed decisions about their healthcare.
Instruct the client that an advance directive is a legal document and must be honored by care providers: The nurse should explain to the client that an advance directive is a legally binding document that guides healthcare decisions, and it must be respected and followed by healthcare providers.
Communicate advance directives status via the medical record and shift report: The nurse should ensure that the client's advance directives status is accurately documented in the medical record and communicated to other members of the healthcare team during shift handoffs. This helps ensure that the client's wishes are known and respected by all involved in their care.
Initiate a power of attorney for health care document: The nurse can assist the client in initiating a power of attorney for healthcare document if the client wishes to appoint someone as their healthcare proxy or agent. This document designates someone to make medical decisions on behalf of the client if they become unable to do so.
The other options listed are not appropriate or accurate in relation to the responsibilities of the nurse regarding advance directives:
Document that the provider discussed-do-not-resuscitate status with the client: While discussing do-not-resuscitate (DNR) status may be part of the advance care planning process, it is not directly related to advance directives as a whole.
Inform the client that an advance directive discontinues further care: This statement is incorrect and misleading. An advance directive does not automatically discontinue care but rather guides the provision of care according to the client's wishes.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["C"]
Explanation
A: The tubing should not be coiled on the bed, especially not above the collection bag, as this can interfere with the drainage of urine and increase the risk of infection.
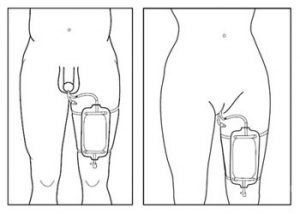
B: The drainage bag should always be kept below the level of the bladder during ambulation to prevent backflow and reduce the risk of infection.
C: Securing the catheter tubing to the lower abdomen (for male clients) or thigh (for female clients) helps to reduce the risk of catheter displacement and trauma. Proper securing also prevents unnecessary tension on the tubing, which can cause urethral irritation.
D:A sterile specimen should be collected from the sampling port of the catheter tubing, not directly from the drainage bag, which could lead to contamination.
Correct Answer is A
Explanation
A- Apply a skin barrier protectant to the site: Using a skin barrier protectant helps shield the peristomal skin from irritation and breakdown caused by gastric contents and formula leakage.
B- Apply water-soluble lubricant to the site: Similarly, applying a water-soluble lubricant to the site is not a routine step in gastrostomy tube site care. Lubricants are typically used during the insertion of the tube or for intermittent tube feedings, but not for routine site care.
C- Tape the tube to the child's cheek: Taping the tube to the child's cheek is not necessary for routine site care. The tube should be secured using a dressing or device designed for gastrostomy tube stabilization, rather than taping it to the cheek.
D.Attaching an extension tube is related to administering feedings or medications rather than the maintenance and care of the gastrostomy site. Site care focuses on protecting the skin and ensuring cleanliness around the tube insertion area.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today