A nurse is assisting with preparing a client who is to have a central venous catheter inserted for the administration of total parenteral nutrition (TPN). Which of the following actions should the nurse take?
Verify the amount of TPN solution the client is receiving every 4 hr.
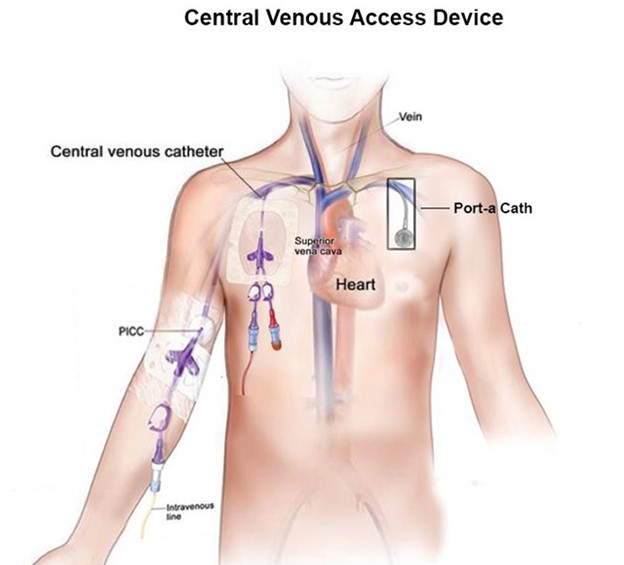
Prepare the client for a chest x-ray to verify catheter placement.
Use clean technique when changing the catheter dressing.
Place the client in Sims' position for catheter insertion.
The Correct Answer is B
When a central venous catheter (CVC) is inserted, it is essential to confirm proper catheter placement to ensure safe and effective administration of TPN and other medications. A chest x-ray is the gold standard method to verify the correct positioning of the CVC tip. It helps determine if the catheter is appropriately positioned in the superior vena cava or another desired location, which minimizes the risk of complications such as pneumothorax or improper medication delivery.
The other options listed are not appropriate actions for the nurse to take in this situation:
- Verifying the amount of TPN solution the client is receiving every 4 hours is a task related to ongoing monitoring of TPN administration, but it is not directly related to the preparation of the client for CVC insertion.
- Using clean technique when changing the catheter dressing is not appropriate for CVC insertion. Sterile technique is required during the insertion of a CVC to minimize the risk of infection.
- Placing the client in Sims' position is not the appropriate position for CVC insertion. The client is typically placed in a supine or Trendelenburg position during the procedure to facilitate access to the central venous system.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Placing soiled dressings in a biohazard trash receptacle is the appropriate practice for disposing of potentially infectious materials. It helps prevent the spread of microorganisms and ensures proper handling and disposal of contaminated items.
Clostridium difficile is a spore-forming bacterium that is not effectively killed by alcohol-based hand rubs. Hand hygiene for C. difficile requires the use of soap and water to thoroughly wash the hands.
Droplet precautions typically require the use of a surgical mask, not a gown and gloves. Gown and gloves are used for contact precautions.
The recommended bleach solution for blood spills is typically a 1:10 dilution, not 1:20. This concentration helps ensure effective disinfection and decontamination of the area.
Correct Answer is A
Explanation
Explanation
A. Write the information at an 8 th grade reading level
Writing the information at an 8th-grade reading level ensures that it is accessible and understandable to a wide range of individuals in the community. Hypertension is a common health condition, and it is important to provide information in a clear and concise manner that can be easily comprehended by the target audience.
Explaining medical terminology using basic, one-syllable in words in (option B) is not recommendable because it may oversimplify the information and potentially undermine the importance of accuracy and precision in healthcare communication.
Using a 12-point font size in (option C) is not recommendable because it is a general guideline for readability, but it is not the most critical aspect when developing a brochure. The readability of the content itself is more important than the specific font size.
D. Presenting information from complex to simple in (option D) is not recommendable because it is not the most effective approach when developing a brochure about hypertension. It is more beneficial to present information in a simple and straightforward manner from the beginning to enhance understanding and engagement.
Therefore, the nurse should write the information at an 8th-grade reading level (option A) to ensure that it is easily accessible and comprehensible for the target audience.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today