A nurse is caring for a client who reports a headache and has a history of a peptic ulcer. Which of the following medications should the nurse administer?
Ketorolac
Acetaminophen
Aspirin
Ibuprofen
The Correct Answer is B
Choice A reason:
Ketorolac is incorrect because it is an NSAID that is used for short-term pain relief. It has a higher risk of causing irritation to the stomach lining and is not recommended for clients with a history of peptic ulcers.
Choice B reason:
Acetaminophen is the correct answer. When caring for a client who reports a headache and has a history of a peptic ulcer, the nurse should administer Acetaminophen. Acetaminophen is an analgesic (pain reliever) and antipyretic (fever reducer) that does not have anti-inflammatory properties. It is a suitable option for pain relief in clients with a history of peptic ulcers because it is less likely to cause irritation to the stomach lining compared to nonsteroidal anti-inflammatory drugs (NSAIDs).
Choice C reason
Aspirin is not appropriate: Aspirin is an NSAID with anti-inflammatory, analgesic, and antipyretic properties. Like other NSAIDs, it can increase the risk of stomach irritation and should be avoided in clients with a history of peptic ulcers.
Choice D reason:
Ibuprofen is not the right option: Ibuprofen is another NSAID commonly used for pain relief and reducing inflammation and fever. Like other NSAIDs, it can irritate the stomach lining and is not recommended for clients with a history of peptic ulcers.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The correct answer is choice D. Speak directly to the client. This is because the nurse should establish eye contact and rapport with the client, not the interpreter, and show respect for the client’s culture and autonomy. The nurse should also use simple and clear language, avoid jargon and slang, and speak in short sentences.
Choice A is wrong because using gestures to convey meaning can be confusing or offensive to some cultures. The nurse should avoid relying on nonverbal communication and ask the interpreter for clarification if needed.
Choice B is wrong because pausing in the middle of sentences can disrupt the flow of communication and make it harder for the interpreter to translate accurately. The nurse should pause at the end of each complete thought or sentence to allow the interpreter to relay the information.
Choice C is wrong because speaking slowly when talking to the interpreter can imply that the interpreter is incompetent or unintelligent. The nurse should speak at a normal pace and tone, and allow enough time for the interpreter to translate.
Correct Answer is C
Explanation
This is a sign of preeclampsia, a serious complication of pregnancy that can cause high blood pressure, proteinuria, and seizures.
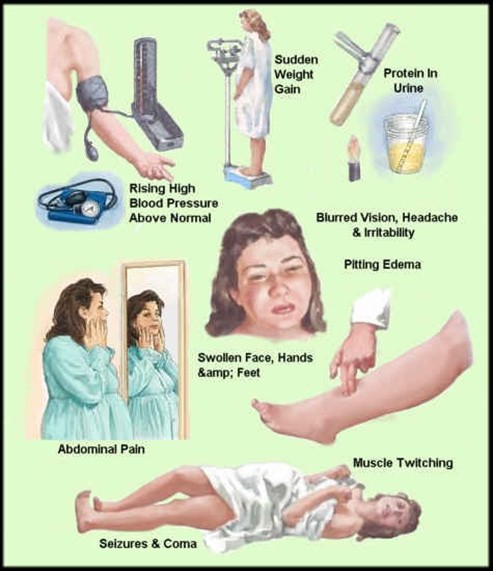
Preeclampsia can affect the placenta, the kidneys, the liver, and the brain of the mother and the fetus. It requires immediate medical attention and may lead to early delivery.
Choice A, bleeding gums, is wrong because it is a common occurrence during pregnancy due to hormonal changes that increase blood flow to the gums. It is not a cause for concern unless it is excessive or accompanied by other symptoms.
Choice B, urinary frequency, is wrong because it is also a normal finding during pregnancy due to the growing uterus putting pressure on the bladder. It is not a sign of infection or kidney problems unless it is associated with pain, burning, or blood in the urine.
Choice D, faintness upon rising, is wrong because it is usually caused by orthostatic hypotension, a drop in blood pressure when changing positions.
This can happen during pregnancy due to the dilation of blood vessels and the increased blood volume. It can be prevented by rising slowly, drinking enough fluids, and avoiding prolonged standing.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today