A nurse is assessing the fontanels of an 8-month-old infant. Which of the following findings should the nurse recognize as an expected finding
The anterior fontanel is open.
Both fontanels are the same size.
The posterior fontanel is open.
Both fontanels show moulding
The Correct Answer is A
Choice A reason
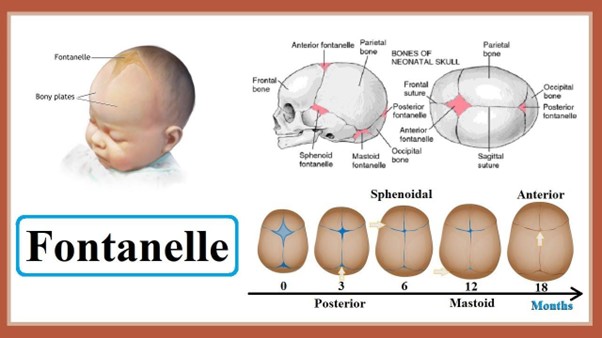
The anterior fontanel is open is the correct answer. An expected finding in an 8-month-old infant is that the anterior fontanel (the soft spot on the top of the baby's head) is open. The fontanelles are spaces between the bones of an infant's skull that allow for the baby's brain to grow and the skull to mould during birth.
The anterior fontanel typically remains open until the baby is around 18 to 24 months old, with the closure process starting sometime after 9 months of age. Therefore, at 8 months of age, it is normal for the anterior fontanel to still be open.
Choice B reason:
Both fontanels are the same size is incorrect. Both fontanels are usually not the same size. The anterior fontanel is larger and diamond-shaped, while the posterior fontanel is smaller and triangular.
Choice C reason:
The posterior fontanel is open is incorrect. The posterior fontanel, located at the back of the baby's head, usually closes earlier than the anterior fontanel. It typically closes within the first few months after birth, so it is not expected to be open at 8 months of age.
Choice D reason
Both fontanels show molding is incorrect. Molding refers to the temporary shaping of the baby's head during birth due to the pressure exerted during the passage through the birth canal. By 8 months of age, the molding typically resolves, and the baby's head should have a more rounded appearance.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
The correct answer is choice A. Limit oral feedings to 30 min in length.
This is because infants with heart failure have difficulty feeding and may become exhausted or dyspneic during prolonged feedings. By limiting the feeding time, the nurse can reduce the energy expenditure and caloric needs of the infant.
Choice B is wrong because weighing the infant every other day is not enough to monitor the fluid status and nutritional intake of the infant. The nurse should weigh the infant daily at the same time using the same scale.
Choice C is wrong because placing the infant in the prone position can compromise the respiratory function and increase the risk of sudden infant death syndrome (SIDS). The nurse should place the infant in a semi-Fowler’s position to facilitate breathing and decrease venous return.
Choice D is wrong because checking the infant’s oxygen saturation every 6 hr is not frequent enough to detect hypoxia or cyanosis. The nurse should monitor the oxygen saturation continuously or at least every 2 hr.
Correct Answer is B
Explanation
Choice A reason:
Explaining the procedure to the client before verifying informed consent is not an appropriate action: While it is essential to explain the procedure to the client and ensure they have a clear understanding of what they are consenting to, this step typically occurs before the informed consent form is presented. The purpose of the informed consent form is to document that the client has received adequate information and has given their consent voluntarily
Choice B reason:
Confirming the client's signature is authentic is the correct action. Verifying the record of informed consent for a client scheduled for surgery involves several important steps. Of these, the nurse's primary responsibility is to ensure that the client's signature on the informed consent form is authentic. This means ensuring that the client themselves or their authorized representative has signed the form willingly and without coercion.
Choice C reason:
Providing information on the informed consent form about the benefits of the surgery is not an appropriate action: The informed consent form typically contains information about the procedure, its risks, possible complications, and alternatives, but it is not the nurse's responsibility to provide this information. The healthcare provider or surgeon is responsible for explaining the details of the surgery to the client before obtaining their consent.
Choice D reason:
Informing the client about the condition that requires treatment is not an appropriate action: The responsibility of informing the client about their medical condition, the need for treatment, and the available options lies with the healthcare provider or surgeon, not the nurse. The nurse may assist in providing information or answering questions, but the primary responsibility for discussing the medical condition lies with the provider.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today