A nurse is caring for a client who is malnourished with poor skin integrity. The nurse should utilize which type of dressing to protect the client's bony prominences?
Foam
Non-adherent
Ace bandage
Hydrocolloid
The Correct Answer is B
A. Foam:
Explanation: Foam dressings are highly absorbent and provide cushioning and protection to wounds. They are suitable for wounds with moderate to heavy drainage. While foam dressings are excellent for wound exudate management, they are not specifically designed for protecting bony prominences or areas with poor skin integrity.
B. Non-adherent:
Explanation: Non-adherent dressings are made from materials that do not stick to the wound bed. They are ideal for fragile skin, bony prominences, or superficial wounds where minimizing trauma during dressing changes is important. Non-adherent dressings are often used for preventing further skin damage in malnourished clients with poor skin integrity.
C. Ace bandage:
Explanation: Ace bandages, or elastic bandages, are primarily used for providing compression and support to injured joints or muscles. They are not designed for protecting bony prominences or fragile skin areas. Using an Ace bandage on a bony prominence could lead to pressure points and skin damage.
D. Hydrocolloid:
Explanation: Hydrocolloid dressings are absorbent and form a gel-like barrier when they come into contact with wound exudate. They provide a moist environment that supports healing and autolytic debridement. Hydrocolloid dressings are suitable for wounds with light to moderate drainage. While they are beneficial for certain wounds, they are not specifically indicated for protecting bony prominences in malnourished clients.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. "Pyelonephritis increases a person's risk for kidney damage." - Pyelonephritis is a bacterial infection of the renal parenchyma and renal pelvis, typically caused by the ascent of bacteria from the lower urinary tract into the kidneys. If left untreated, it can lead to kidney damage, including scarring of the renal tissue and impaired kidney function.
B. "Pyelonephritis is an infection of the lower urinary tract." - This statement is incorrect. Pyelonephritis specifically involves the upper urinary tract, affecting the kidneys. In contrast, infections of the lower urinary tract (such as cystitis) affect the bladder and urethra.
C. "Pyelonephritis often causes no symptoms in affected clients." - This statement is incorrect. Pyelonephritis typically presents with symptoms such as fever, chills, flank pain, painful urination (dysuria), and frequent urination. Clients with pyelonephritis usually experience noticeable symptoms.
D. "Pyelonephritis is most often caused by Staphylococcus saprophyticus." - This statement is incorrect. While Staphylococcus saprophyticus is a common cause of urinary tract infections, pyelonephritis is more commonly caused by gram-negative bacteria, such as Escherichia coli, which often ascend from the lower urinary tract into the kidneys.
Correct Answer is A
Explanation
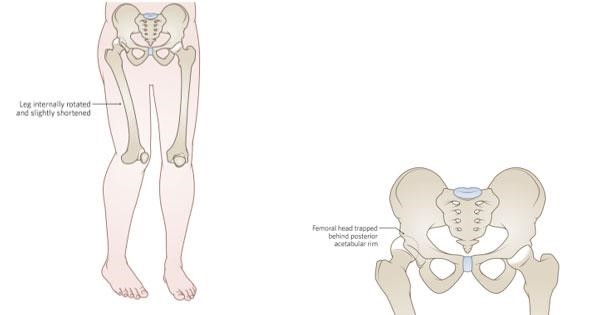
A. Right hip dislocation: In a hip dislocation, the head of the femur is forced out of the acetabulum, which is the socket in the pelvis. This can cause a noticeably shorter leg, hip deformity, and acute pain. Imaging might not show a fracture in the case of a dislocation.
B. Right hip contusion: A hip contusion is a bruise on the hip, usually caused by a direct blow or trauma. While it can cause pain and swelling, it typically does not result in a noticeably shorter leg or hip deformity.
C. Right hip strain: Hip strain refers to damage to the muscles or tendons around the hip joint due to overuse or sudden twisting movements. While it can cause pain, it does not typically lead to a noticeable leg shortening or hip deformity.
D. Right hip osteoarthritis: Osteoarthritis is a degenerative joint disease that can affect the hip joint. It leads to joint pain and stiffness but does not usually cause a noticeable leg shortening or acute deformity unless there are severe complications, which are not mentioned in the scenario.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today