A nurse is caring for a client who has a prescription for total parental nutrition (TPN).
Which of the following routes of administration should the nurse use?
Central venous access device.
Midline catheter.
Subcutaneous.
Intraosseous.
The Correct Answer is A
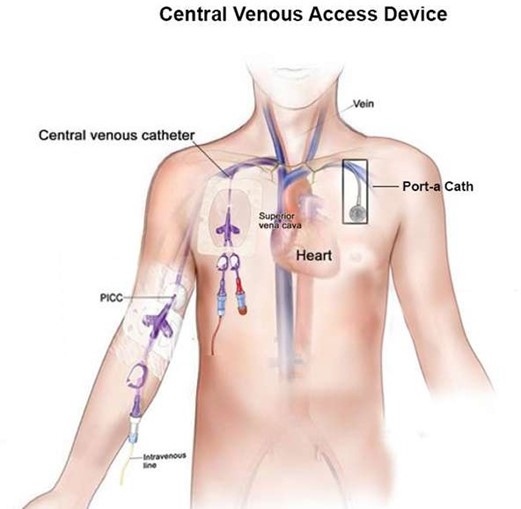
Total parenteral nutrition (TPN) is a highly concentrated solution that provides nutrients to the body intravenously.
It is typically administered through a central venous access device, such as a central venous catheter or a peripherally inserted central catheter (PICC), because it can irritate the walls of smaller veins.
Choice B is wrong because Midline catheter, is not an appropriate route for TPN administration because it is not a central venous access device.
Choice C is wrong because Subcutaneous, is not an appropriate route for TPN administration because it is not given intravenously.
Choice D is wrong because Intraosseous, is not an appropriate route for TPN administration because it is typically used in emergency situations when intravenous access cannot be obtained.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Anaphylaxis is a severe, potentially life-threatening allergic reaction that can occur within seconds or minutes of exposure to an allergen, such as penicillin.
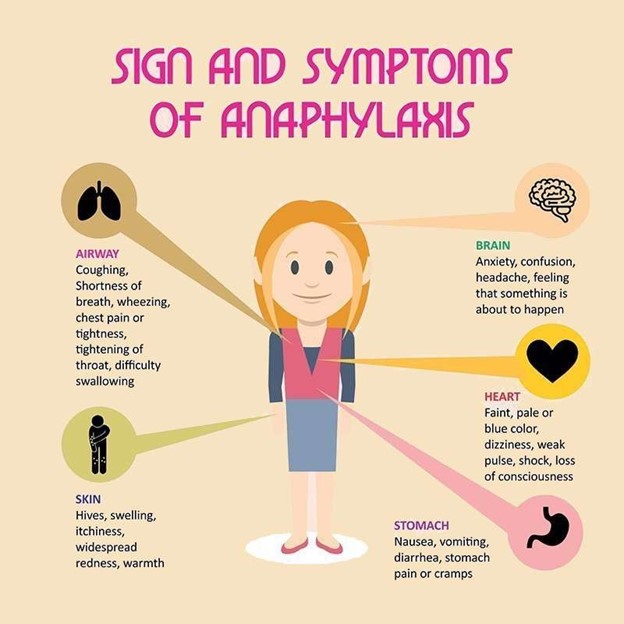
One of the symptoms of anaphylaxis is wheezing, which is caused by the constriction of the airways and a swollen tongue or throat.
Choice A is wrong because hypertonia (increased muscle tone) is not a known symptom of anaphylaxis.
Choice C is wrong because urinary retention (inability to completely empty the bladder) is not a known symptom of anaphylaxis.
Choice D is wrong because increased blood pressure is not a known symptom of anaphylaxis; in fact, anaphylaxis can cause a sudden drop in blood pressure.
Correct Answer is A
Explanation
Total parenteral nutrition (TPN) is a method of administration of essential nutrients to the body through a central vein.

TPN solutions are customized for each client’s needs, including the exact amount of calories and nutrients necessary for total nutritional needs.
Monitoring the client’s weight daily is important to determine if nutritional goals are being met and to assess fluid volume status.
Choice B is wrong because TPN solutions are concentrated and can cause thrombosis of peripheral veins, so they require a central venous catheter and should not be hung to gravity to infuse.
Choice C is wrong because TPN solution should not be titrated to blood pressure.
Choice D is wrong because the client’s blood glucose level should be monitored more frequently than weekly when receiving TPN.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today