A nurse is caring for a 2-day-old newborn who was born at 35 weeks of gestation.
Which of the following actions should the nurse take
Diagnostic results
Escherichia coli infection resulting in necrotizing enterocolitis Hgb 10g/dL
Platelet count 50,000 mm
WBC count 4,000 mm3
The Correct Answer is A
The nurse should insert an orogastric decompression tube with low wall suction. The newborn has Escherichia coli infection resulting in necrotizing enterocolitis, which can cause abdominal distention, decreased activity level, and bloody stools. The newborn also has a superficial rash on the abdominal wall, which may indicate a bacterial infection. The presence of a fist clenching, thrashing, and crying during light palpation of the
abdomen may indicate pain caused by bowel distention. An orogastric decompression tube with low wall suction can help decompress the bowel and relieve abdominal distention.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
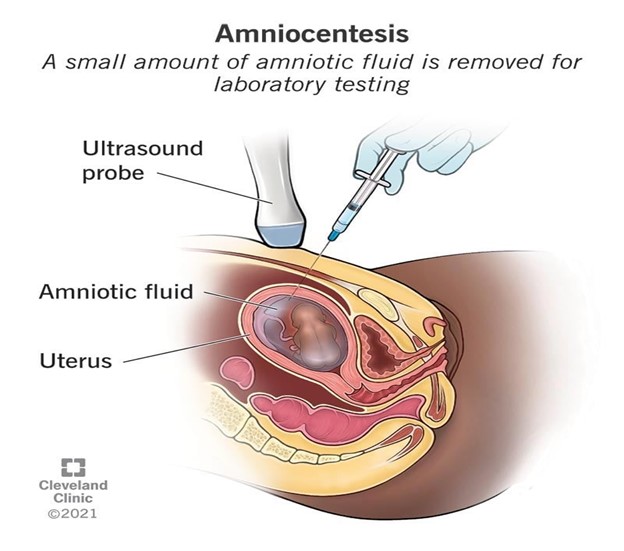
The nurse should explain to the client that amniocentesis is a diagnostic test that is performed between 15 and 20 weeks of gestation to determine if the fetus has genetic or congenital disorders. While the procedure can also determine the sex of the fetus, this is not typically the primary reason for the test. The nurse should clarify any misconceptions the client has about the procedure and provide education on its purpose, risks, and benefits. The nurse should also assess the client's understanding of the information provided and address any questions or concerns the client may have.
Correct Answer is B
Explanation
A. This option is incorrect because the development of breast tissue in newborns is not directly related to the mother’s hormone levels during pregnancy. Newborns typically have breast buds regardless of maternal hormone variations.
B. A flat areola with no breast bud is a characteristic finding in preterm newborns. Breast tissue development is one of the physical markers used to assess gestational age, and the lack of a breast bud is an indicator of immaturity, suggesting a preterm gestational age.
C. Ambiguous secondary sex characteristics are not related to the presence or absence of breast buds in newborns. This option focuses on sexual development rather than gestational markers.
D. A flat areola with no breast bud is a normal finding in preterm infants and does not indicate a congenital anomaly. This condition is expected in preterm newborns based on their developmental stage.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today