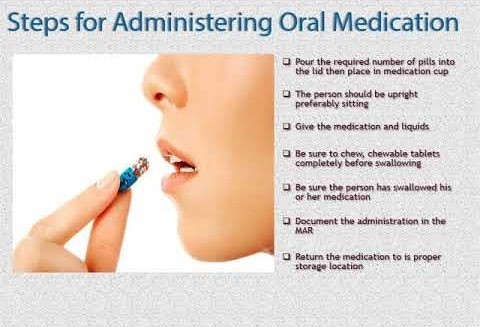
A nurse is administering a client's morning oral medications. Which of the following actions should the nurse take?
Verify the medication three times with the medication administration record.
Document medication administration prior to administering medication.
Administer time-critical medication 60 min before or after the scheduled time.
Identify the client by using one identifier before giving the medication.
The Correct Answer is A
When administering oral medications, the nurse should verify the medication three times with the medication administration record to ensure that the correct medication is being given to the correct client at the correct time. This is known as the "three checks" and is an important step in preventing medication errors.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The correct action to take in this situation is to place a pillow or cushion under the child's head.
This will help protect the child from injuring their head during the seizure.
It is important not to turn the child onto their back during a seizure, as this can obstruct the airway and potentially lead to respiratory distress.
Restraining the child's upper extremities is also not recommended, as it can cause injury to the child or the person trying to restrain them.
Placing a padded tongue blade or any object in the child's mouth is no longer recommended during a seizure. Doing so can cause injury to the child's mouth or teeth and is not necessary for seizure management.
Correct Answer is ["C","D","E","F"]
Explanation
c, d, e, and f.
a.An advance directive does not automatically discontinue further care. It simply provides guidance to healthcare providers on the client's wishes for medical treatment. It is important for the nurse to explain this to the client and ensure that they understand the purpose of an advance directive.
b. While nurses can provide information and support the client in understanding the importance of having a power of attorney for healthcare, initiating such documents is typically not within the scope of nursing practice. This task usually requires legal guidance and formalities that go beyond nursing responsibilities.
c.Accurate documentation is crucial in healthcare. If a provider discusses do-not-resuscitate (DNR) status with a client, it must be documented in the client's medical record to ensure that all healthcare team members are aware of the client’s wishes.
d. Provide the client with writen information about advance directives: It is important for the nurse to provide the client with writen information about advance directives, including their rights and options for creating an advance directive. This information should be provided in a clear and understandable manner.
e. Communicate advance directives status via the medical record and shift report: The nurse should communicate the client's advance directives status to other members of the healthcare team via the medical record and shift report. This ensures that everyone involved in the client's care is aware of the client's wishes and can provide care that is consistent with those wishes.
f. Instruct the client that an advance directive is a legal document and must be honored by care providers: The nurse should instruct the client that an advance directive is a legal document that must be honored by care providers. This ensures that the client understands the importance of their advance directive and can advocate for their wishes if necessary.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today