A nurse is caring for a newly admitted older adult client.
Nurses' Notes
Day 1, 12:00:
Transferred to the medical-surgical unit from the emergency department (ED) for continued care following a closed reduction and immobilization of a fracture of the right arm. Accompanied by an adult child.
Client in visibly soiled night clothes with multiple stains, including what appears to be dried blood. Hair, teeth, and fingernails unclean. Strong body odor noted. Bruising of various stages noted around upper arms, back, shoulders, and neck area.
The client is soft-spoken, speaks almost in a whisper, and does not make eye contact with the nurse.
The client looks at their child before answering the nurse's questions and, when asked how the injury occurred, mumbles "I don't know. Ask them." The client's child states, "He gets confused sometimes. I can answer your questions."
Which of the following interventions should the nurse recommend to include in the client's plan of care?
Select all that apply.
Tell the client's child that they will be reported for maltreatment of the client.
Ask the client's child to provide details regarding the client's fractured arm.
Discuss respite care options with the client's child.
Speak to the client privately.
Provide legal advice to the client regarding the power of attorney.
Correct Answer : B,C,D
It is not appropriate for the nurse to threaten the client's child with reporting for maltreatment without further assessment and evidence.
Asking the client's child to provide details regarding the client's fractured arm will provide additional information about the client's injury and help the nurse assess the potential for abuse or neglect.
Discussing respite care options with the client's child may help alleviate any caregiver stress or burden, and ensure the client's continued care and safety.
Speaking to the client privately will help establish trust and rapport, and allow the client to disclose any
concerns or issues that they may not feel comfortable sharing in front of their child.
Providing legal advice regarding power of attorney is not within the scope of nursing practice and should be referred to a legal professional. Additionally, the client's capacity to make decisions and appoint a power of attorney should be assessed before providing such advice.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
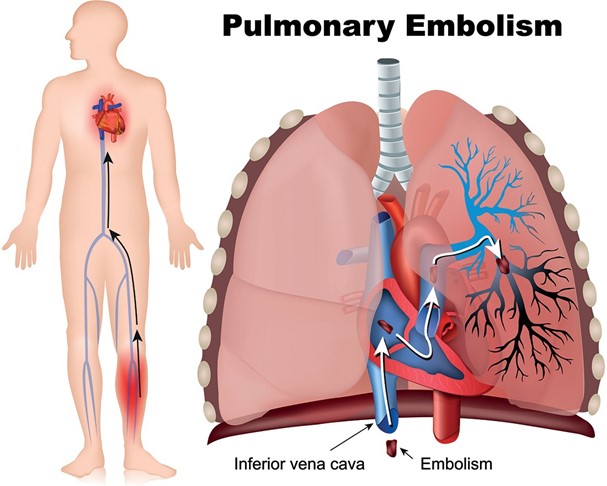
Pain in the calf can be a potential symptom of deep vein thrombosis (DVT), which is a serious complication after surgery. Monitoring the client's pulse oximetry can help assess for signs of decreased oxygenation, which may indicate a possible clot or compromised circulation. A decrease in oxygen saturation can be an early indicator of a potential DVT-related complication, such as a pulmonary embolism. Monitoring the pulse oximetry can provide valuable information for timely intervention and management.
Instructing the client to massage the calf gently is not advisable without further assessment and evaluation. Massaging the calf can potentially dislodge a clot if one is present, leading to further complications. It is important to rule out DVT through appropriate diagnostic measures before providing specific instructions for calf massage.
Maintaining the leg in a dependent position while in bed can potentially worsen the symptoms and increase the risk of venous stasis. Elevating the affected leg, rather than maintaining it in a dependent position, can help improve venous return and reduce pain or swelling.
Applying a cold compress to the client's calf is not recommended without further assessment. Heat or cold therapy should be applied based on the underlying cause of the pain. In the case of potential DVT, applying a cold compress can increase vasoconstriction and potentially worsen the condition. It is essential to investigate the cause of the pain first and consult with the healthcare provider before initiating any specific therapies or interventions.
Correct Answer is D
Explanation
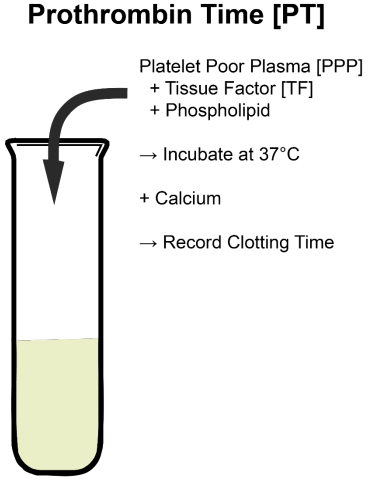
Prothrombin time.
Explanation:
When a client is prescribed warfarin, monitoring the prothrombin time (PT) and the International Normalized Ratio (INR) is crucial. Warfarin is an anticoagulant medication that affects the clotting ability of the blood by inhibiting vitamin K-dependent clotting factors. Monitoring the prothrombin time and INR helps determine the client's blood's ability to clot and the appropriate dosage of warfarin to maintain the desired therapeutic range.
Option a (Triiodothyronine) is a thyroid hormone and is not directly related to warfarin therapy.
Option b (Blood urea nitrogen) is a measure of kidney function and is also not directly related to warfarin therapy.
Option c (Arterial blood gases) is a measure of oxygen and carbon dioxide levels in the blood and is not related to warfarin therapy.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today