A nurse in a provider's office is caring for a client who reports pruritus and reddened, oozing lesions on her lower leg. The nurse should suspect which of the following disorders?
Contact dermatitis
Tinea pedis
Pediculosis
Alopecia
The Correct Answer is A
Choice A rationale: Pruritus (itching) and reddened, oozing lesions are common symptoms of contact dermatitis, which can result from exposure to irritants or allergens.
Choice B rationale: Tinea pedis, or athlete's foot, typically presents with scaling, redness, and itching between the toes.
Choice C rationale: Pediculosis refers to infestation with lice, which may cause itching and small, red papules, but it usually does not involve oozing lesions.
Choice D rationale: Alopecia refers to hair loss and is not typically associated with pruritus and oozing lesions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A rationale: Herpes zoster itself is not easily spread, but the varicella-zoster virus can be transmitted to individuals who have not had chickenpox or the varicella vaccine.
Choice B rationale: While the virus can be spread through contact with the fluid from shingles blisters, it can also be spread by respiratory droplets from the infected person.
Choice C rationale: Postherpetic neuralgia is a common complication of herpes zoster (shingles), and it involves persistent pain in the affected area even after the lesions have healed.
Choice D rationale: This statement is accurate, but it does not address the persistent pain (postherpetic neuralgia) that can occur after the lesions resolve.
Correct Answer is ["A","C","D"]
Explanation
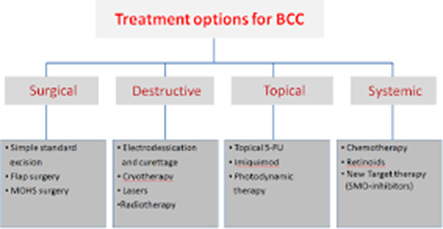
Choice A rationale: radiation therapy is one of the possible management options for basal cell carcinoma (BCC) that uses high-energy rays to kill the cancerous cells.
Choice B rationale: this is incorrect since topical corticosteroids are ineffective in BCC management and may worsen the patient’s condition by suppressing their immune system.
Choice C rationale: micrographic surgery can be used in BCC management and it involves the removal of thin layers of skin to a point where no cancer cells can be detected.
Choice D rationale: this is appropriate and involves the use of electric current to burn off the cancer cells.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today