A nurse is assessing a client who is brought to the emergency room with burn injuries. Which of the following findings should the nurse identify as a deep partial-thickness burn?
The burned area is yellow in color with severe edema.
The burned area is black in color and pain is absent.
The burned area is pink in color with blisters present.
The burned area is red in color with soft eschar present.
The Correct Answer is D
Choice A Reason: The burned area is yellow in color with severe edema is not a finding of a deep partial-thickness burn, but a superficial partial-thickness burn. A superficial partial-thickness burn involves the epidermis and the upper layer of the dermis, causing pain, redness, swelling, and blistering.
Choice B Reason: The burned area is black in color and pain is absent is not a finding of a deep partial-thickness burn, but a full-thickness burn. A full-thickness burn involves the epidermis, dermis, and underlying tissues, causing necrosis, charred skin, and loss of sensation.
Choice C Reason: This description aligns with a superficial partial-thickness (first-degree or mild second-degree) burn rather than a deep partial-thickness burn. Superficial partial-thickness burns involve the epidermis and the upper portion of the dermis. These burns appear pink or red, often accompanied by moisture and blister formation due to fluid leakage from damaged capillaries. They are painful because nerve endings remain intact. Healing occurs within 10 to 21 days without significant scarring.
Choice D Reason: Deep partial-thickness burns extend deeper into the dermis, damaging a larger portion of skin structures, including sweat glands and hair follicles. These burns typically appear red or white and may have a soft eschar (dead tissue), which differentiates them from more superficial burns that do not develop eschar. Unlike full-thickness burns, nerve endings remain partially intact, so the patient may still experience some pain. These burns take more than 21 days to heal and often require skin grafting to prevent complications such as contractures or hypertrophic scarring.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
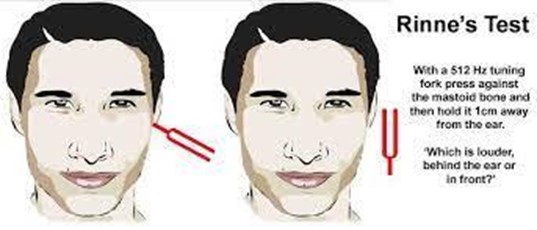
Choice A Reason: This is incorrect because earphones are not used in the Rinne test. The Rinne test compares air conduction and bone conduction of sound using a tuning fork.
Choice B Reason: This is incorrect because electrodes are not used in the Rinne test. Electrodes are used in electroencephalography (EEG), which measures brain activity.
Choice C Reason: This is incorrect because a probe is not used in the Rinne test. A probe is used in tympanometry, which measures the pressure and mobility of the eardrum.
Choice D Reason: This is correct because a tuning fork is used in the Rinne test. The tuning fork is placed on the mastoid process behind the ear and then moved near the ear canal to compare the sound perception.
Correct Answer is D
Explanation
Choice A reason: This is incorrect because the nurse should not include this in teaching. Massaging the affected side multiple times a day can trigger an acute onset of trigeminal neuralgia. Trigeminal neuralgia is a condition that causes severe pain in one or more branches of the trigeminal nerve (cranial nerve V), which innervates the face. The pain can be triggered by touch, pressure, or movement of the face. The nurse should advise the client to avoid touching or stimulating the affected side.
Choice B reason: This is incorrect because the nurse should not include this in teaching. Applying ice directly to
the skin can trigger an acute onset of trigeminal neuralgia. Trigeminal neuralgia can be triggered by temperature changes or cold stimuli on the face. The nurse should advise the client to avoid exposure to cold air or wind and to protect their face with a scarf or mask.
Choice C reason: This is incorrect because the nurse should not include this in teaching. Providing pureed consistency foods can trigger an acute onset of trigeminal neuralgia. Trigeminal neuralgia can be triggered by chewing, swallowing, or talking. The nurse should advise the client to eat soft foods that do not require much chewing and to avoid hot or spicy foods that can irritate the mouth.
Choice D reason: This is correct because the nurse should include this in teaching. Considering alternative therapies such as yoga, biofeedback or meditation can help prevent triggering an acute onset of trigeminal neural
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today