A nurse is assisting a client with a visual impairment to use the restroom. Which of the following actions will the nurse take to prevent complications?
Increase her voice when speaking to the client
Lower the bed rails before lowering the bed
Use hand gestures to point to where the client will walk
Stand slightly in front and to one side of the client
The Correct Answer is D
Choice A reason: This is incorrect because increasing her voice when speaking to the client may not prevent complications, but rather annoy or offend the client. The nurse should not assume that a client with a visual impairment has a hearing impairment as well unless it is confirmed by assessment or history. The nurse should speak in a normal tone and volume and identify herself by name and role.
Choice B reason: This is incorrect because lowering the bed rails before lowering the bed may increase the risk of complications, such as falls or injuries. The nurse should keep the bed rails up until the client is ready to get out of bed and lower them only when necessary. The nurse should also lock the wheels of the bed and adjust it to a comfortable height for the client.
Choice C reason: This is incorrect because using hand gestures to point to where the client will walk may not prevent complications, but rather confuse or frustrate the client. The nurse should not use visual cues or gestures that are meaningless to a client with a visual impairment. The nurse should use verbal directions and descriptions instead, such as "The restroom is on your left, about 10 steps away."
Choice D reason: This is correct because standing slightly in front and to one side of the client can prevent complications, such as collisions or falls. The nurse should guide the client by offering her arm or shoulder for support and walking slightly ahead of him or her. The nurse should also warn the client about any obstacles or changes in terrain, such as stairs, doors, or rugs.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: This is incorrect because drawing with crayons may be too childish or frustrating for a client with moderate Alzheimer's. Crayons may also pose a choking hazard or cause messes. The nurse should provide activities that are suitable for the client's cognitive and functional level, as well as their interests and preferences.
Choice B Reason: This is incorrect because dangling ribbons or a mobile may be too stimulating or confusing for a client with moderate Alzheimer's. These items may also trigger agitation or wandering behaviors. The nurse should provide activities that are calming and familiar for the client.
Choice C Reason: This is correct because listening to music, watching TV, or videos can be enjoyable and beneficial for a client with moderate Alzheimer's. Music can evoke memories, emotions, and positive responses. TV or videos can provide entertainment, education, and socialization. The nurse should choose music, TV shows, or videos that are appropriate and meaningful for the client.
Choice D Reason: This is incorrect because board games may be too complex or challenging for a client with moderate Alzheimer's. Board games may require memory, concentration, logic, or strategy skills that the client may have lost. The nurse should provide activities that are simple and easy for the client to follow.
Correct Answer is B
Explanation
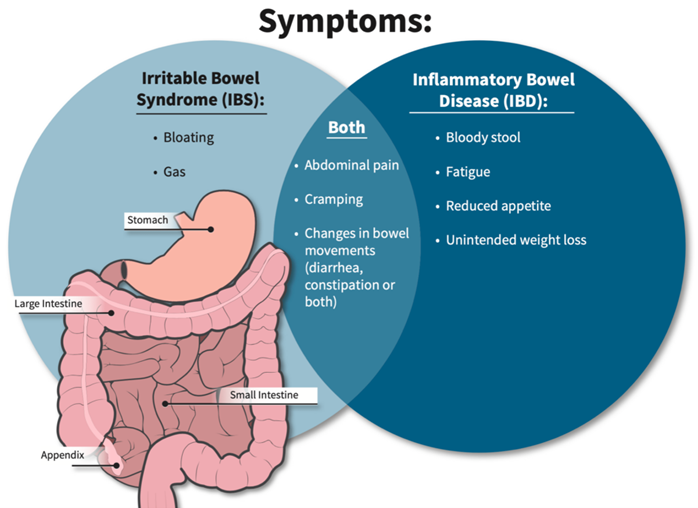
Choice A reason: This is correct because eating frequent small meals can help the client with IBS to avoid overloading the digestive system and triggering diarrhea. The nurse should advise the client to eat slowly chew well, and avoid foods that are spicy, fatty, or gas-producing.
Choice B reason: This is incorrect because increasing the intake of leafy greens and other sources of dietary fiber can worsen diarrhea by increasing stool bulk and motility. The nurse should advise the client to limit or avoid high-fiber foods, such as whole grains, fruits, vegetables, nuts, and seeds, during acute flare-ups of IBS. The client can gradually reintroduce fiber when the symptoms subside.
Choice C reason: This is correct because increasing fluids can help the client with IBS to prevent dehydration and electrolyte imbalance caused by diarrhea. The nurse should advise the client to drink at least 8 glasses of water per day and avoid caffeinated, alcoholic, or carbonated beverages that can irritate the bowel or cause gas.
Choice D reason: This is correct because taking prescribed medications on schedule can help the client with IBS to regulate bowel patterns and reduce diarrhea. The nurse should instruct the client on how to use medications, such as antidiarrheals, antispasmodics, or probiotics, as ordered by the provider. The nurse should also monitor the client for any adverse effects or interactions of the medications.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today