A nurse enters the room of a client with type 1 diabetes mellitus and finds the client difficult to arouse. The client's skin is warm and flushed and the pulse and respiratory rate are increased from the client's baseline. The nurse would first take which action?
Assist the RN to prepare an intravenous (IV) insulin infusion.
Give the client 4 oz of orange juice.
Check the client's capillary blood glucose.
Assist the RN to administer 50% dextrose.
The Correct Answer is C
Choice A Reason: Assisting the RN to prepare an IV insulin infusion is not the first action that the nurse should take, as it may not be appropriate for the client's condition without knowing the blood glucose level.
Choice B Reason: Giving the client 4 oz of orange juice is not the first action that the nurse should take, as it may worsen the client's condition if the blood glucose level is high.
Choice C Reason: Checking the client's capillary blood glucose is the first action that the nurse should take, as it helps to determine if the client has hyperglycemia or hypoglycemia and guides the appropriate intervention.
Choice D Reason: Assisting the RN to administer 50% dextrose is not the first action that the nurse should take, as it may be harmful for the client if the blood glucose level is high.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: Side lying on the affected eye is not the correct position for the client after cataract surgery, as it may increase intraocular pressure and cause bleeding or damage to the surgical site.
Choice B Reason: Supine is not the correct position for the client after cataract surgery, as it may cause fluid accumulation and swelling in the eye.
Choice C Reason: Prone is not the correct position for the client after cataract surgery, as it may cause pressure and friction on the eye.
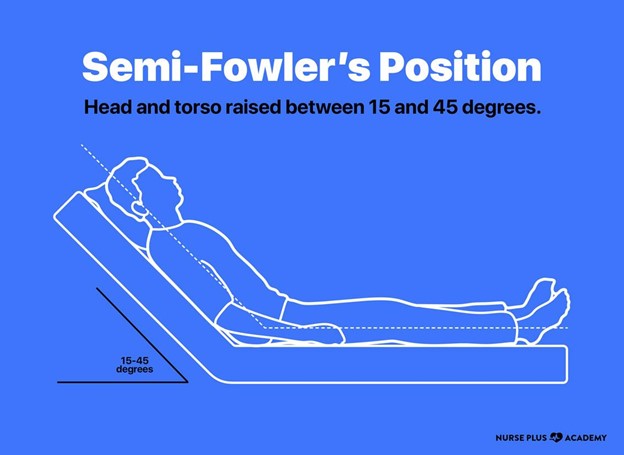
Choice D Reason: Semi Fowler's is the correct position for the client after cataract surgery, as it helps to reduce intraocular pressure and promote drainage and healing of the eye.
Correct Answer is D
Explanation
Choice A Reason: Telling the client that this is to be expected after surgery is not the first action that the nurse should take, as it may indicate a complication such as increased intraocular pressure, hemorrhage, or infection.
Choice B Reason: Placing the client in a supine position is not the first action that the nurse should take, as it may worsen the pain and increase intraocular pressure.
Choice C Reason: Documenting the findings is not the first action that the nurse should take, as it may delay the intervention and outcome.
Choice D Reason: Notifying the surgeon is the first action that the nurse should take, as it indicates that the client needs immediate evaluation and treatment to prevent vision loss or permanent damage to the eye.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today