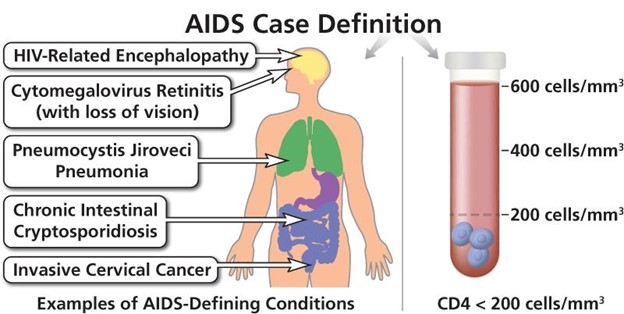
The nurse is participating in a care planning conference for a patient with acquired immunodeficiency syndrome (AIDS). What is the nurse's highest priority in providing care to this client?
Instituting measures to prevent infection.
Providing emotional support.
Identifying risk factors related to contracting AIDS.
Discussing the cause of AIDS.
The Correct Answer is A
Choice A Reason: Instituting measures to prevent infection is the highest priority in providing care to this client, as AIDS impairs the immune system and makes the client susceptible to opportunistic infections that can be life-threatening.
Choice B Reason: Providing emotional support is an important aspect of providing care to this client, but it is not the highest priority, as it does not address the physical needs of the client.
Choice C Reason: Identifying risk factors related to contracting AIDS is not relevant for providing care to this client, as it does not help to improve the current condition or prevent complications.
Choice D Reason: Discussing the cause of AIDS is not essential for providing care to this client, as it does not affect the treatment or prognosis of the disease.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
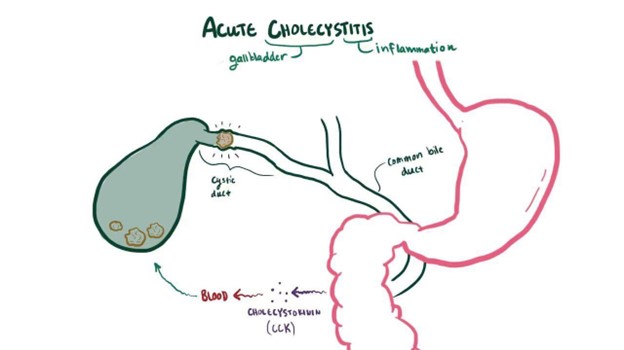
Choice A Reason: Ice cream is not a good food choice for a client who has cholecystitis, as it is high in fat and may trigger gallbladder pain or inflammation.
Choice B Reason: Blueberry muffin is not a good food choice for a client who has cholecystitis, as it may contain butter, oil, or eggs that are high in fat and may aggravate gallbladder symptoms.
Choice C Reason: Macaroni and cheese is not a good food choice for a client who has cholecystitis, as it is high in fat and cholesterol and may cause gallstone formation or obstruction.
Choice D Reason: Roast turkey is a good food choice for a client who has cholecystitis, as it is low in fat and high in protein and may help to prevent gallbladder attacks.
Correct Answer is C
Explanation
Choice A Reason: Cold skin is not a common finding in hyperthyroidism, but it may indicate hypothyroidism or other conditions such as hypothermia or shock.
Choice B Reason: Weight gain is not a common finding in hyperthyroidism, but it may indicate hypothyroidism or other conditions such as Cushing's syndrome or edema.
Choice C Reason: Tachycardia is a common finding in hyperthyroidism, as the increased thyroid hormone level causes the heart rate and cardiac output to increase.
Choice D Reason: Anorexia is not a common finding in hyperthyroidism, but it may indicate other conditions such as depression, infection, or cancer.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today