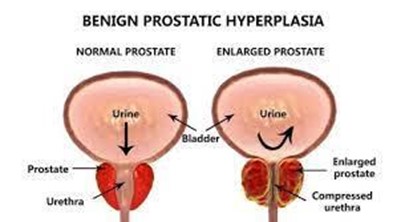
A nurse is caring for a client who has benign prostatic hyperplasia (BPH). Which of the following findings should the nurse expect?
Painful urination
Decreased urinary stream
Critically elevated prostate-specific antigen (PSA) level
Urge incontinence
The Correct Answer is B
Choice A Reason: Painful urination is not a common finding in BPH, but it may indicate a urinary tract infection or bladder stones.
Choice B Reason: Decreased urinary stream is a common finding in BPH, as the enlarged prostate compresses the urethra and obstructs the flow of urine.
Choice C Reason: Critically elevated PSA level is not a common finding in BPH, but it may indicate prostate cancer or prostatitis.
Choice D Reason: Urge incontinence is not a common finding in BPH, but it may indicate an overactive bladder or neurogenic bladder.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: Instructing the client to increase fluid intake is not the most appropriate nursing action, as it does not address the cause or severity of the bleeding.
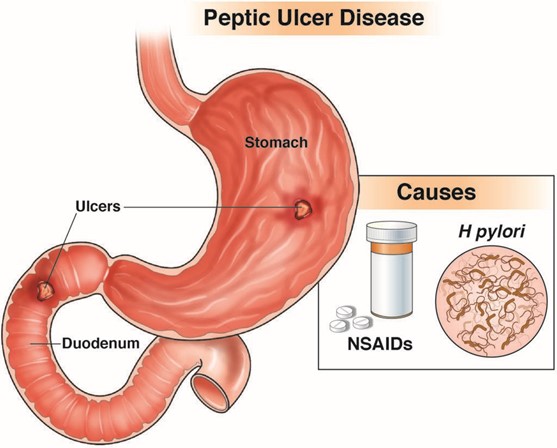
Choice B Reason: Notifying the health care provider is the most appropriate nursing action, as it indicates that the client may have a bleeding ulcer that requires immediate evaluation and treatment.
Choice C Reason: Advising the client to take iron rich foods is not the most appropriate nursing action, as it does not prevent or correct anemia or bleeding.
Choice D Reason: Documenting the findings is not the most appropriate nursing action, as it does not initiate any intervention or outcome.
Correct Answer is A
Explanation
Choice A Reason: Buffalo hump and moon face are physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, as they indicate fat redistribution and accumulation due to excess cortisol production.
Choice B Reason: Dry, scaly skin and cold intolerance are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hypothyroidism, which affects the metabolism and skin condition.
Choice C Reason: Dry, sticky mucous membranes and hypovolemia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate dehydration or diabetes insipidus, which affect the fluid balance and urine output.
Choice D Reason: Exophthalmos and tachycardia are not physical assessment findings that the nurse would expect to observe in a client with Cushing's syndrome, but they may indicate hyperthyroidism, which affects the eye protrusion and heart rate.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today