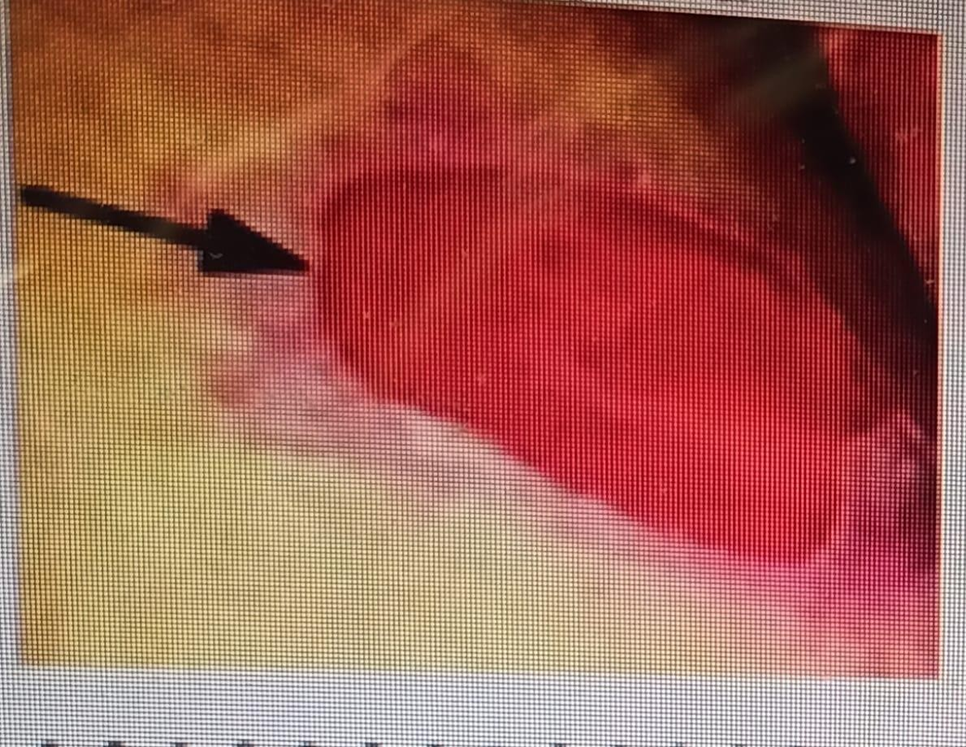
A nurse begins her shift and is completing her first turn of the night. While turning, she also assesses her patient's skin. When she turns her patient she finds the following wound on her coccyx. How should she document the following wound? (The base of the wound is muscle, with some subcutaneous tissue)

Stage III Pressure Ulcer
Stage IV Pressure Ulcer
Stage II Pressure Ulcer
Unstageable Ulcer
The Correct Answer is B
Choice A rationale: Stage III pressure ulcers involve full-thickness tissue loss with visible fat but do not extend to the underlying muscle.
Choice B rationale: Stage IV pressure ulcers involve full-thickness tissue loss with exposed muscle, bone, or other structures.
Choice C rationale: Stage II pressure ulcers involve partial-thickness skin loss but do not extend into the deeper layers.
Choice D rationale: Unstageable ulcers have a base covered by slough or eschar, making it difficult to assess the depth of tissue involvement. In this case, the wound's base is described as muscle, indicating a stage IV pressure ulcer.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["1.5"]
Explanation
Number of tablets = total dose/ tablet strength
= 30/20
= 1.5 tablets
Correct Answer is B
Explanation
Choice A rationale: Stage I pressure ulcers consist of non-blanching erythema with an intact epidermis unlike in the above picture.
Choice B rationale: This is correct since Stage II pressure ulcers involve partial-thickness skin loss but do not extend into the deeper layers as shown in the image above.
Choice C rationale: Stage IV pressure ulcers involve full-thickness tissue loss with exposed muscle, bone, or other structures.
Choice D rationale: Stage III pressure ulcers involve full-thickness tissue loss with visible fat but do not extend to the underlying muscle.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today