A nurse at a provider's office is collecting physical data from an older adult client. Which of the following images should the nurse identify as an example of an expected age-related change?
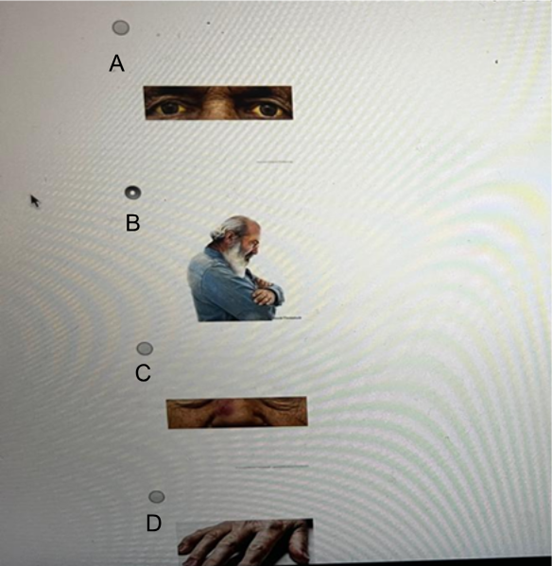
A
B
C
D
The Correct Answer is D
A. Close-up of eyes with yellow sclera: Could indicate jaundice or liver dysfunction, which is not an expected part of aging and requires further evaluation.
B. Older adult man with a rounded back and head tilted forward: Suggests kyphosis, which can occur with aging but is usually linked to osteoporosis or vertebral fractures, not considered an inevitable, expected change.
C. Close-up of nose with a reddish-purple spot (possible bruise): Might result from trauma, coagulopathy, or medication side effects like anticoagulants, not a routine age-related change.
D. Hands with prominent veins, thin skin, and wrinkles: Thinning skin due to decreased subcutaneous fat. Wrinkles from reduced skin elasticity. Prominent veins due to loss of skin turgor and connective tissue. These are all normal physical findings in older adults.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. Mark the length to be inserted on the tube with tape: Marking the insertion length is important to ensure correct placement, but this step should occur after assessing which nare to use and preparing the client.
B. Instruct the client to hyperextend her neck: Hyperextending the neck is not recommended during NG tube insertion; instead, the client should slightly flex the neck to facilitate tube passage.
C. Place a water-based lubricant on the tip of the tube: Lubricating the tube reduces discomfort and eases insertion, but this step comes after selecting the nostril and preparing the client.
D. Compare the patency of the client’s nares: Assessing which nostril is more patent is the first priority to ensure the tube is inserted through the nare that offers the least resistance, reducing trauma and improving comfort during insertion.
Correct Answer is D
Explanation
A. Close-up of eyes with yellow sclera: Could indicate jaundice or liver dysfunction, which is not an expected part of aging and requires further evaluation.
B. Older adult man with a rounded back and head tilted forward: Suggests kyphosis, which can occur with aging but is usually linked to osteoporosis or vertebral fractures, not considered an inevitable, expected change.
C. Close-up of nose with a reddish-purple spot (possible bruise): Might result from trauma, coagulopathy, or medication side effects like anticoagulants, not a routine age-related change.
D. Hands with prominent veins, thin skin, and wrinkles: Thinning skin due to decreased subcutaneous fat. Wrinkles from reduced skin elasticity. Prominent veins due to loss of skin turgor and connective tissue. These are all normal physical findings in older adults.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today