A macrosomic infant is born after a difficult forceps-assisted delivery.
After stabilization, the infant is weighed, and the birth weight is 4550 g (9 lbs, 6 ounces). The nurse’s most appropriate action is to:
Leave the infant in the room with the mother.
Take the infant immediately to the nursery.
Perform a gestational age assessment to determine whether the infant is large for gestational age.
Monitor blood glucose levels frequently and observe closely for signs of hypoglycemia.
The Correct Answer is D
choice D. Monitor blood glucose levels frequently and observe closely for signs of hypoglycemia. This is because a macrosomic infant (a newborn who’s much larger than average) is at risk of developing low blood sugar levels after birth, especially if the mother has diabetes. Hypoglycemia can cause neurological damage in the newborn, so it is important to detect and treat it promptly.
Choice A is wrong because leaving the infant in the room with the mother without monitoring the blood glucose levels may miss signs of hypoglycemia and delay treatment.
Choice B is wrong because taking the infant immediately to the nursery may separate the infant from the mother and interfere with breastfeeding, which can help prevent hypoglycemia.
Choice C is wrong because performing a gestational age assessment to determine whether the infant is large for gestational age is not urgent and does not address the risk of hypoglycemia.
Normal ranges for blood glucose levels in term infants are 2.6 mmol/L or higher at any time. A blood glucose level of 2.5 mmol/L or less is considered hypoglycemic.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
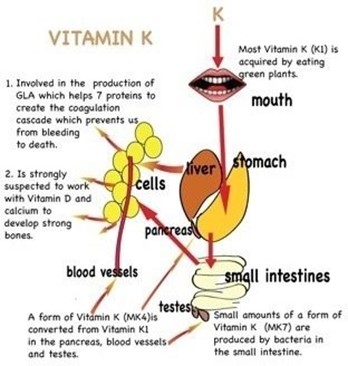
Bacteria that synthesize vitamin K is not present in the newborn’s intestinal tract. Vitamin K is essential for blood clotting, and newborns are at risk of bleeding problems due to their lack of vitamin K. Therefore, vitamin K is given by injection to prevent hemorrhagic disease in the newborn.
Choice A is wrong because most mothers do not have a diet deficient in vitamin K, and vitamin K deficiency in newborns is not related to the maternal diet.
Choice B is wrong because vitamin K does not prevent the synthesis of prothrombin in the liver, but rather enhances it. Prothrombin is a clotting factor that requires vitamin K for its production.
Choice D is wrong because the supply of vitamin K is not inadequate for at least 3 to 4 months, but rather for a few days until the newborn’s intestinal bacteria start producing it.
Correct Answer is A
Explanation
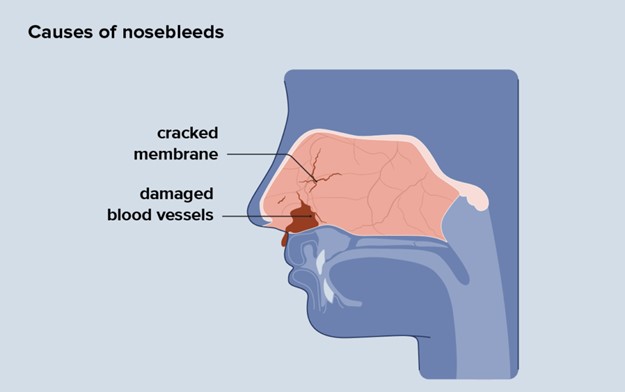
This is a normal respiratory change in pregnancy caused by elevated levels of estrogen. Estrogen increases blood flow and causes the nasal mucosa to swell, leading to congestion and nosebleeds. This condition is called pregnancy rhinitis and affects up to 20% of pregnant women.
Choice B is wrong because this is not an abnormal cardiovascular change, and the nosebleeds are not an ominous sign. They are usually harmless and do not affect the pregnancy outcome.
Choice C is wrong because there is no evidence that the woman is a victim of domestic violence.
This is a serious accusation that should not be made without proper assessment and screening.
Choice D is wrong because there is no indication that the woman has been using cocaine intranasally. Cocaine use can cause nasal damage and bleeding, but it can also have other signs and symptoms such as agitation, euphoria, dilated pupils, increased heart rate and blood pressure, and risk of miscarriage or preterm labor.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today