As relates to rubella and Rh issues, nurses should be aware that:.
Breastfeeding mothers cannot be vaccinated with the live attenuated rubella virus.
Women should be warned that the rubella vaccination is teratogenic and that they must avoid pregnancy for 1 month after vaccination.
Rh immune globulin is safely administered intravenously because it cannot harm a nursing infant.
Rh immune globulin boosts the immune system and thereby enhances the effectiveness of vaccinations.
The Correct Answer is B
The presence or absence of anxiety is a noninvasive assessment that the RN would perform to evaluate the patient’s psychological status and possible signs of hypovolemic shock.
Anxiety can indicate reduced cerebral perfusion due to blood loss and low blood pressure.
Choice A is wrong because pulse oximetry is a noninvasive assessment that the RN would perform to measure the oxygen saturation of the patient’s blood, not the circulatory status.
Choice B is wrong because heart sounds are a noninvasive assessment that the RN would perform to auscultate the cardiac rhythm and rate of the patient, not the circulatory status.
Choice C is wrong because arterial pulses are a noninvasive assessment that the RN would perform to palpate the strength and quality of the patient’s peripheral pulses, not the circulatory status.
Choice D is wrong because skin color, temperature, and turgor are noninvasive assessments that the RN would perform to observe the skin integrity and hydration of the patient, not the circulatory status.
Normal ranges for pulse oximetry are 95% to 100%, for heart rate, are 60 to 100 beats per minute, and for blood pressure are 120/80 mmHg.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","C"]
Explanation
The child’s care should include adequate hydration and pain management. The management of an acute event of a vaso-occlusive crisis is the use of potent analgesics (opioids), rehydration with normal saline or Ringer’s lactate, treatment of malaria (whether symptomatic or not) using artemisinin combination therapy, and the use of oxygen via face mask, especially for acute chest syndrome.
Choice A is wrong because correction of acidosis is not a specific intervention for the vaso- occlusive crisis.
Acidosis may occur as a complication of sickle cell disease, but it is not the primary cause of the crisis.
Choice D is wrong because the administration of heparin is not recommended for the vaso-occlusive crisis.
Heparin is an anticoagulant that may increase the risk of bleeding and does not prevent or treat the sickling process.
Normal ranges for hemoglobin are 11.5 to 15.5 g/dl for children after 2 years of age.
Normal ranges for reticulocyte count are 0.5% to 1.5% for adults and 0.5% to 2.5% for children.
Correct Answer is A
Explanation
choice A. Surfactant improves the ability of your baby’s lungs to exchange oxygen and carbon dioxide.
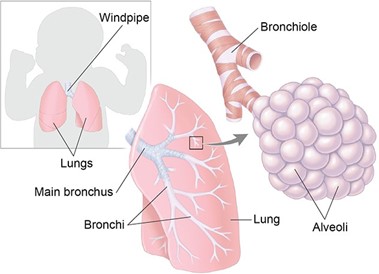
Surfactant is a substance that coats the inner surface of the alveoli, the tiny air sacs in the lungs.
It reduces the surface tension of the alveoli and prevents them from collapsing during exhalation.
Premature infants often lack enough surfactant, which leads to respiratory distress syndrome (RDS).
Artificial surfactant is given to these infants to help them breathe more easily. Choice B is wrong because surfactant has nothing to do with sedation.
Sedation is a state of reduced consciousness induced by drugs. Surfactant does not affect the level of consciousness of the infant.
Choice C is wrong because surfactant is not used to reduce episodes of periodic apnea.
Periodic apnea is a condition where the infant stops breathing for a short time, usually due to immature brainstem function.
Surfactant does not affect the brainstem or the control of breathing.
Choice D is wrong because surfactant is not used to fight a possible respiratory tract infection. Surfactant does not have any antibacterial or antiviral properties.
Surfactant is used to treat RDS, which is caused by a lack of surfactant, not by an infection.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today