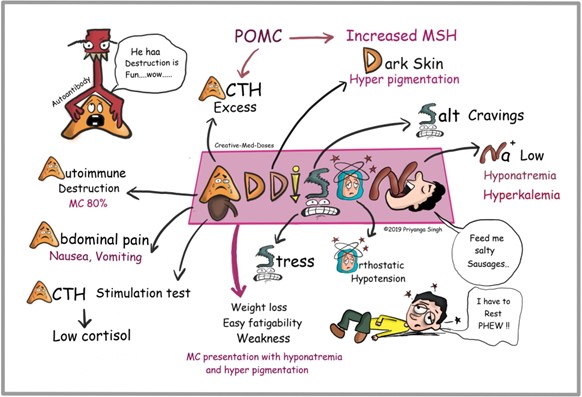
A client with Addison's disease becomes weak, confused, and dehydrated following the onset of an acute viral infection. The client's laboratory values include: sodium 129 mEq/L (129 mmol/L), glucose 54 mg/dl (2.97 mmol/L) and potassium 5.3 mEq/L (5.3 mmol/L).
When reporting the findings to the healthcare provider, the nurse anticipates a prescription for which intravenous medication?
Reference Ranges
- Sodium [Reference Range: Adult 136 to 145 mEq/L (136 to 145 mmol/L)
- Glucose (Reference Range: 0 to 50 years: 74 to 106 mg/dl. (4.1 to 5.9 mmol/L))
- Potassium [Reference Range: 3.5 to 5.0 mEq/L (3.5 to 5.0 mmol/L)
Broad spectrum antibiotic.
Regular insulin.
Hydrocortisone.
Potassium chloride.
The Correct Answer is C
The client with Addison's disease is experiencing weakness, confusion, and dehydration, which can be indicative of an adrenal crisis. The low sodium level (129 mEq/L) and low glucose level (54 mg/dl) further support this suspicion. An acute viral infection can trigger an adrenal crisis in individuals with Addison's disease.
Intravenous hydrocortisone, a glucocorticoid, is the treatment of choice for managing an adrenal crisis. It helps to replenish cortisol levels and stabilize the client's condition.
Hydrocortisone helps in restoring the body's stress response and regulating electrolyte and glucose levels.
A broad-spectrum antibiotic may be necessary if there is evidence of a bacterial infection, but it does not directly address the symptoms associated with Addison's disease.
Regular insulin is used for managing high blood glucose levels in conditions such as diabetes, but in this case, the client has low glucose levels, so insulin is not the appropriate intervention.
Potassium chloride is a medication used to treat low potassium levels (hypokalemia), but the client's potassium level is within the reference range (5.3 mEq/L). Therefore, potassium chloride is not indicated in this situation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A) Incorrect - While a salad includes vegetables and fruits, it may not provide sufficient protein for wound healing.
B) Incorrect - Vegetable soup and crackers might not provide enough protein compared to other options.
C) Incorrect - While a peanut butter sandwich includes some protein, soda and cookies are not rich sources of protein.
D) Correct- A tuna fish sandwich is a good source of protein. Protein is essential for wound healing as it supports tissue repair and regeneration. The choice of a tuna fish sandwich along with chips and ice cream suggests a balanced meal with adequate protein content, which aligns with the teaching of a high protein diet to promote wound healing.
Correct Answer is ["B","C","D"]
Explanation
A) Incorrect- Standard precautions are used for all clients to prevent the spread of infections.
However, in the case of MRSA, contact precautions are needed due to the risk of direct transmission through physical contact.
B) Correct- Monitoring the white blood cell count is important to assess for signs of infection, as an elevated count might indicate an ongoing inflammatory response.
C) Correct- Foul-smelling drainage from an incision with suspected MRSA indicates a potential infection. Contact precautions are appropriate for MRSA, which include wearing gloves and gowns when entering the client's room to prevent the spread of the bacteria.
D) Correct- Sending wound drainage for culture and sensitivity helps identify the specific microorganisms causing the infection and guides appropriate antibiotic treatment.
E) Incorrect- A low-bacteria diet is not relevant to the situation. MRSA is caused by a bacterium, not by dietary factors. The focus should be on infection control measures and appropriate medical interventions.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today