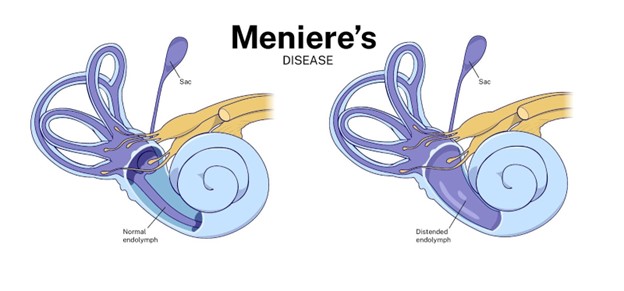
A client admitted with an acute exacerbation of Ménière's disease asks the student nurse why he was prescribed diphenhydramine. Which response by the student nurse requires correction by the primary nurse?
"Ménière's disease is caused by an allergic response."
"This medication can help offset the nauseous feeling."
"Anticholinergics will help you rest."
"This medication can help reduce vomiting episodes."
The Correct Answer is A
Choice A Reason: This is incorrect because Ménière's disease is not caused by an allergic response. Ménière's disease is a disorder of the inner ear that causes vertigo, tinnitus, hearing loss, and a feeling of fullness in the ear. The exact cause of Ménière's disease is unknown, but it may be related to fluid imbalance, infection, trauma, or autoimmune reaction.
Choice B Reason: This is correct because diphenhydramine can help offset the nauseous feeling. Diphenhydramine is an antihistamine that blocks histamine receptors in the brain and inner ear, which can reduce nausea and vomiting associated with vertigo.
Choice C Reason: This is correct because anticholinergics will help you rest. Anticholinergics are a class of drugs that block acetylcholine receptors in the brain and body, which can have sedative effects and reduce motion sickness. Diphenhydramine has anticholinergic properties.
Choice D Reason: This is correct because diphenhydramine can help reduce vomiting episodes. As mentioned above, diphenhydramine can reduce nausea and vomiting by blocking histamine receptors in the brain and inner ear.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because administering medications and electrolytes is not the primary purpose of inserting a nasogastric tube for a client with acute peritonitis. Medications and electrolytes can be given through other routes, such as IV or oral.
Choice B Reason: This is incorrect because dilating the stomach as a presurgical preparation is not a relevant Reason for inserting a nasogastric tube for a client with acute peritonitis. Dilating the stomach may be done before some types of gastric surgery, but it does not apply to peritonitis.
Choice C Reason: This is incorrect because stating that you will not be able to eat for several days is not an adequate explanation for inserting a nasogastric tube for a client with acute peritonitis. This statement does not address the rationale or the benefits of the procedure. It may also cause anxiety and resentment in the client.
Choice D Reason: This is the correct choice because removing secretions and decompressing the stomach is the main Reason for inserting a nasogastric tube for a client with acute peritonitis. Peritonitis is an inflammation of the peritoneum, the membrane that lines the abdominal cavity. It can cause abdominal distension, pain, nausea, and vomiting. A nasogastric tube can suction out the gastric contents and reduce the pressure and irritation in the abdomen.
Correct Answer is A
Explanation
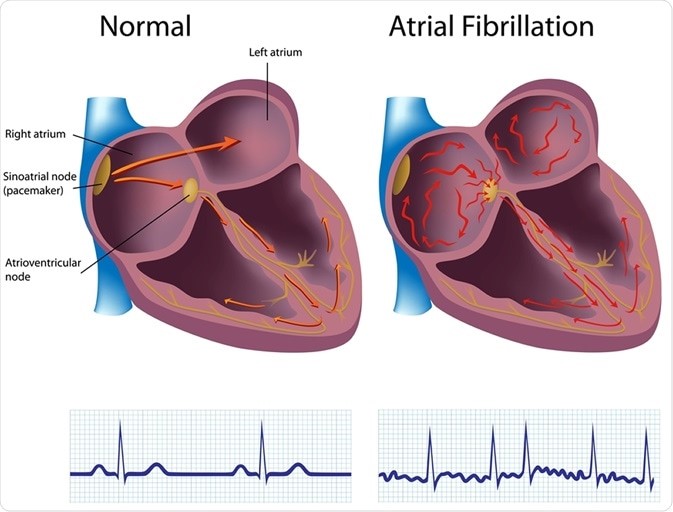
Choice A reason: This is the correct answer because atrial fibrillation is the risk factor that puts the client at
the highest risk for embolic stroke. Atrial fibrillation is an irregular and rapid heart rate that causes poor blood flow and blood pooling in the heart chambers. This can lead to the formation of blood clots that can travel to the brain and block an artery, causing an embolic stroke.
Choice B reason: This is incorrect because hypertension is not the risk factor that puts the client at
the highest risk for embolic stroke. Hypertension is high blood pressure that puts stress on the blood vessels and increases the risk of bleeding or rupture. This can lead to a hemorrhagic stroke, but not an embolic stroke.
Choice C reason: This is incorrect because diabetes is not the risk factor that puts the client at
the highest risk for embolic stroke. Diabetes is a condition that causes high blood sugar levels and damages the blood vessels and nerves. This can lead to poor circulation and increased risk of infection and ulcers, but not an embolic stroke.
Choice D reason: This is incorrect because alcohol abuse is not the risk factor that puts the client at
the highest risk for embolic stroke. Alcohol abuse is excessive consumption of alcohol that affects liver function and blood clotting factors. This can lead to liver disease and bleeding disorders, but not an embolic stroke.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today