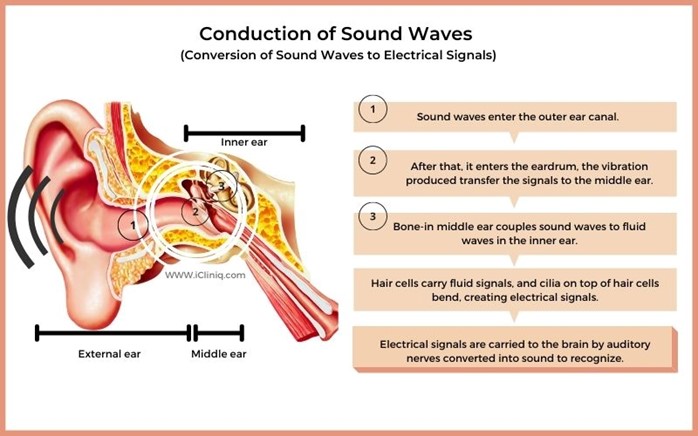
A nurse is caring for a client who has progressive presbycusis. Which of the following actions should the nurse take?
Use sign language when communicating with the client.
Speak loudly and into the client's good ear.
Speak directly to the client in a normal, clear voice.
Sit by the client's side and speak very slowly.
The Correct Answer is C
Choice A reason: This is incorrect because using sign language when communicating with the client is not an appropriate action for the nurse to take. Sign language is a form of communication that uses hand gestures, facial expressions, and body movements. It is not a universal language and requires training and practice. The nurse should not assume that the client knows or prefers sign language unless they have indicated so.
Choice B reason: This is incorrect because speaking loudly and into the client's good ear is not an appropriate action for the nurse to take. Speaking loudly can distort the sound quality and cause discomfort or irritation to the client. Speaking into the client's good ear can also create a sense of imbalance and isolation. The nurse should speak at a normal volume and tone, and face the client directly.
Choice C reason: This is the correct answer because speaking directly to the client in a normal, clear voice is an appropriate action for the nurse to take. Speaking directly to the client can help them see the nurse's mouth movements and facial expressions, which can enhance understanding and communication. Speaking in a normal, clear voice can help convey the message clearly and respectfully.
Choice D reason: This is incorrect because sitting by the client's side and speaking very slowly is not an appropriate action for the nurse to take. Sitting by the client's side can make it difficult for them to see the nurse's face and hear their voice. Speaking very slowly can also make the message unclear and patronizing. The nurse should sit in front of the client and speak at a normal pace.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: This is incorrect because encouraging coughing and deep breathing can increase intracranial pressure (ICP), which is the pressure inside the skull that can affect brain function. Coughing and deep breathing can increase blood flow and oxygen demand to the brain, which can worsen cerebral edema. The nurse should suction the patient as needed and maintain a patent airway.
Choice B Reason: This is incorrect because positioning the patient with knees and hips flexed can increase ICP by reducing venous drainage from the head. The nurse should position the patient with neck and body in alignment and avoid extreme flexion or extension of any joints.
Choice C Reason: This is incorrect because performing nursing interventions once an hour can disturb the patient's sleep and increase ICP by stimulating brain activity. The nurse should cluster nursing interventions and provide quiet and dark environment to promote rest and reduce stress.
Choice D Reason: This is correct because keeping the head of the bed elevated to 30 degrees can decrease ICP by facilitating venous drainage from the head and reducing cerebral blood volume. The nurse should monitor the patient's blood pressure and pulse to ensure adequate cerebral perfusion.
Correct Answer is ["A","B","D"]
Explanation
Choice A Reason: This is correct because melanoma is a type of skin cancer that arises from melanocytes, which are cells that produce pigment. Melanoma lesions are often irregular in shape and color, and may have different shades of brown or black.
Choice B Reason: This is correct because melanoma is a very aggressive and invasive type of skin cancer that can spread quickly to other parts of the body through the blood or lymphatic system. Melanoma has a high mortality rate if not detected and treated early.
Choice C Reason: This is incorrect because warm and red skin around a lesion may indicate inflammation or infection, but not necessarily melanoma. Melanoma lesions may have other signs, such as bleeding, itching, or ulceration.
Choice D Reason: This is correct because melanoma is associated with exposure to ultraviolet (UV) radiation from sunlight or artificial sources, such as tanning beds. UV radiation can damage the DNA of melanocytes and cause them to grow abnormally.
Choice E Reason: This is incorrect because melanoma lesions are usually not painful unless they are ulcerated or infected. Pain may be a sign of other types of skin conditions, such as burns, blisters, or cuts.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today